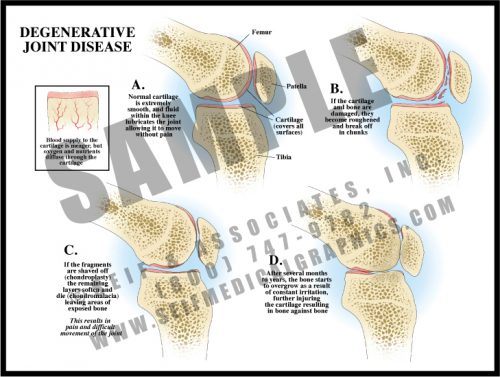
- Degenerative joint disease is a result of normal activity and is found in most people as they get older; it develops more rapidly and more severely in the case of joint trauma.
- Articular surfaces are covered with glassy-smooth cartilage. As the cartilage disintegrates over time (chondromalacia), it flakes off until the bone is eventually exposed.
- If bone starts to rub against bone, it reacts by forming more bone in the form of osteophytes. This is a very painful condition and when severe enough, requires joint replacement.
- Degenerative joint disease is frequently called osteoarthritis; rheumatoid arthritis is an autoimmune disease with very different causes and a slightly different set of symptoms.
-
-
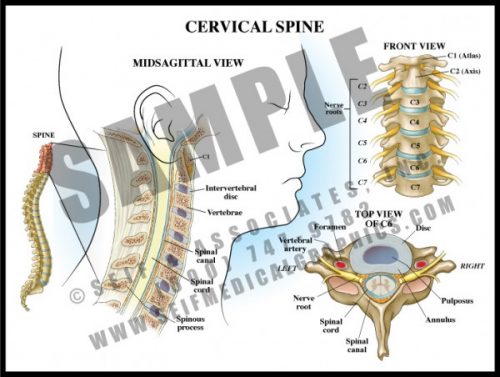
- The 7 vertebrae of the cervical spine help support the skull and protect the spinal cord as it exits the cranium to pass downward through the spinal canal.
- The transverse processes each have a small hole through which the vertebral arteries pass to join to form the basilar artery supplying the posterior and deep portions of the brain and brainstem.
- The cervical nerve roots form the brachial plexus which supplies sensation and movement to the upper extremities.
- Degenerative joint disease and disc disease are very common in the cervical spine, leading to arm and hand pain and dysfunction requiring decompression and sometimes fusion.
-
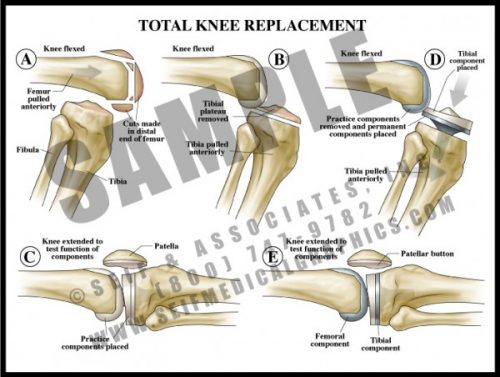
- One of the more common surgical procedures, diseased bone and articular surfaces (usually from either trauma and/or degenerative joint disease) are surgically removed.
- Most knee prostheses are made of a strong metal with a durable plastic overlay to serve as a joint surface.
- As with any bony prosthesis, these can be either cemented into place or have a roughened surface which allows bone to grow into the surface.
- All three units (femoral, tibial and patellar) can be inserted together or individually, depending upon the specific needs of the patient.
-
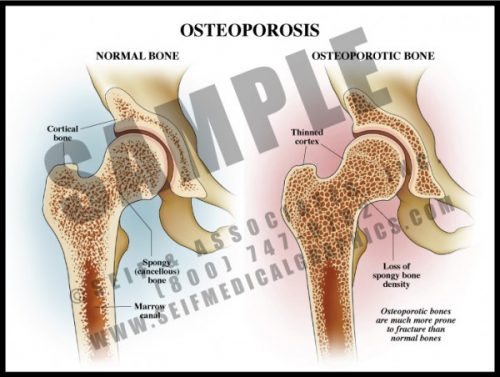
- A common condition, particularly among elderly women, osteoporosis is the reduction of bone density.
- Osteoporosis affects both the dense cortical portion on the outside of a bone and the spongy bone inside.
- Causes include age, low body mass, family history, smoking, malnutrition, alcoholism, insufficient physical activity and certain medications and toxins. It is also associated with a number of chronic diseases.
- The primary risk is that of fracture, particularly of the hip, a potentially devastating event in the elderly. In severely osteoporotic patients, healing may be slow and insufficient.
- Treatment depends on the cause but includes medication, dietary changes, and exercise.
-
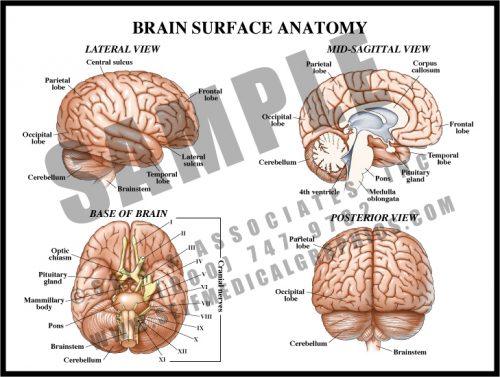
- The surface of the brain has multiple folds, or gyri, separated by sulci. While many of these are specific to a particular individual, some are constant and serve as landmarks for functional control.
- The cerebrum is the large, rounded portion of the brain and is the site of higher functions. The cerebellum and brainstem control more basic functions like heart rate, balance, and respiration.
- The cranial nerves mostly originate in the brainstem and exit the skull via foramina in the base of the skull (see M1). The optic nerves originate in the occipital lobes, travel along pathways inside the brain matter, and exit anteriorly.
- The corpus callosum is a group of myelin-covered neuronal fibers (white matter) which connect the right side of the brain with the left.
-
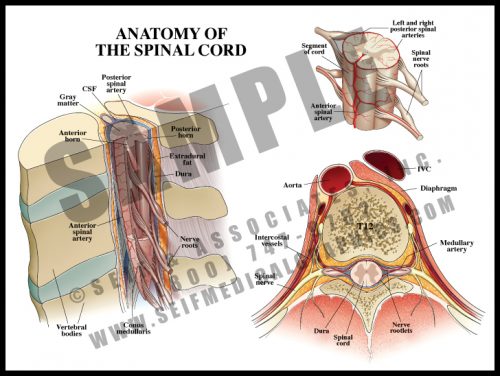
- The spinal cord lies within the spinal canal, formed by the vertebral bodies and the bony arch formed by the pedicles and laminae (see M6).
- The cord and its terminal nerves, the cauda equina, lie within the dural sac, a tough membranous structure filled with cerebrospinal fluid bathing and protecting the cord.
- The spinal cord itself ends at the level of the first lumbar vertebra, but nerve roots travel inside the dural sac to exit at lower levels; these roots form the cauda equina (”horse’s tail”).
- Blood supply comes from the segmental branches of the aorta, traveling along the nerve root to emerge as the anterior spinal artery running in the front midline of the cord; there are two parallel vessels along the back surface of the cord. There is also a generous venous plexus within the canal.
-
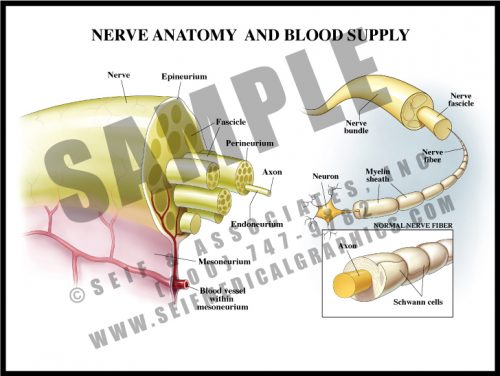
- Nerves are composed of multiple fibers which in turn are composed of many, many axons. Each successive grouping of fibers is surrounded by connective tissue.
- Axons are the long branches of nerves cells which transmit electrochemical impulses from one nerve to another or to and from target organs.
- The axons are surrounded by myelin, a kind of insulating material formed by oligodendrocytes. In diseases in which myelin is destroyed, electrochemical conduction is impossible, and even if the nerve fibers do not die, they are ineffective.
- Blood vessels travel through the mesoneurium and then divide into capillaries within the nerve to deliver oxygen and nutrients.
- Nerves are vulnerable to trauma, reduced oxygen levels, and diabetes.
-
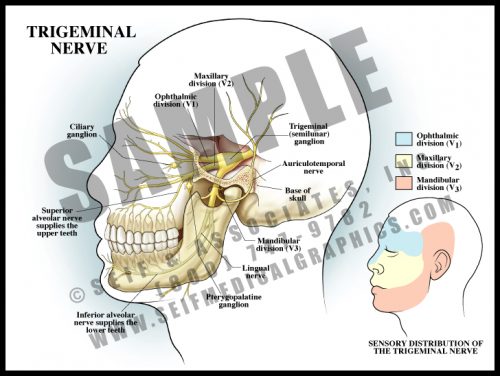
- The semilunar ganglion of the trigeminal nerve lies deep within the skull. The three branches of the nerve leave through large separate openings in the base of the skull.
- The trigeminal nerve is the 5th cranial nerve. Its three portions are the ophthalmic nerve controlling sensation to the upper face, the maxillary nerve controlling sensation to the mid-face, and the mandibular nerve supplying sensation to the lower face and the skin around and above the ear. Each of the branches supplies both soft tissue and bone.
- All large ganglia in the body can harbor certain viruses. Oral herpes infections “hibernate” within the semilunar ganglion, traveling down the nerve roots to the mouth when the virus is activated by stress.
-
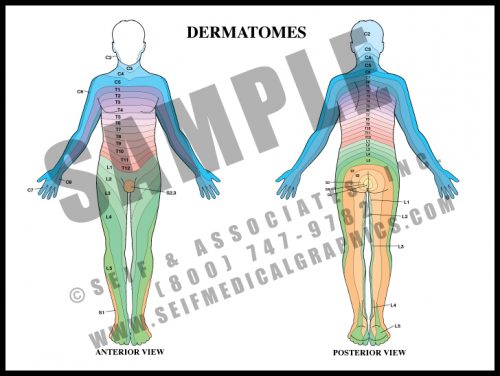
- Dermatomes are strips of skin which are supplied by the nerve roots. If there is numbness or pain along a dermatome, it is a sign of damage or irritation of a specific nerve root, where the root exits the spinal cord and vertebral column. This is known as radiculopathy.
- Soon after the cervical and lumbosacral nerves leave the cord, they join and separate several times (plexi) before reaching their target organs. Nerve fibers to a given muscle may come from several different nerve roots. The skin sensory supply, however, remains directly associated with the root alone.
- Radicular pain usually occurs with compression of the nerve in the foramen, the hole by which the nerve exits the spinal canal.
-
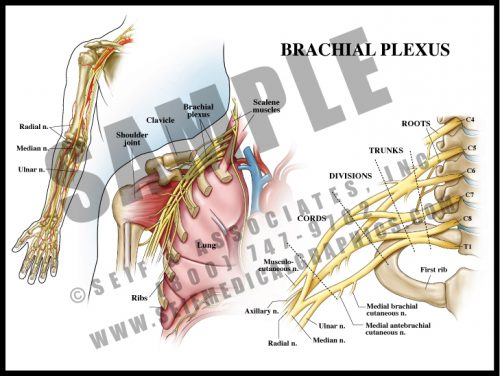
- The nerve roots of the lower cervical spinal cord split and merge several times before supplying the arm and hand.
- The brachial plexus lies over the first rib and behind the clavicle. It is intimately related to the subclavian/brachial artery and passes between the scalene muscles of the neck.
- The plexus is divided into roots, trunks, divisions, cords and terminal branches. By looking at the anatomical distribution of pain or dysfunction, it is possible to determine the location of a brachial plexus lesion.
- Brachial plexopathy can occur during delivery with or without shoulder dystocia, and from thoracic outlet syndrome.
-
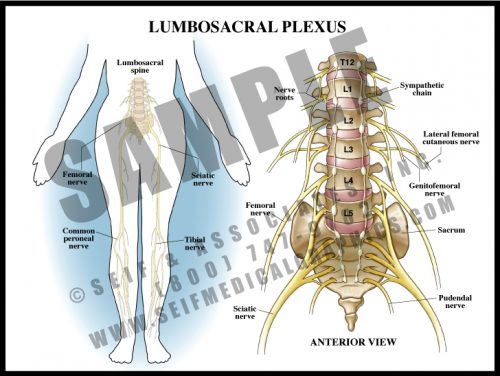
- Analogous to the brachial plexus, the lumbosacral plexus is a series of nerve convergences and separations which ultimately combine into several large terminal nerves.
- Plexi form a protective mechanism in that if one nerve root is damaged, a particular muscle might be weakened, but function would not be completely lost.
- The terminal nerves in the legs generally follow the course of the deep vasculature.
- Terminal sensory nerves to the feet are particularly vulnerable to diabetes, resulting in peripheral diabetic neuropathy. This frequently contributes to foot infections and the need for amputation.
-
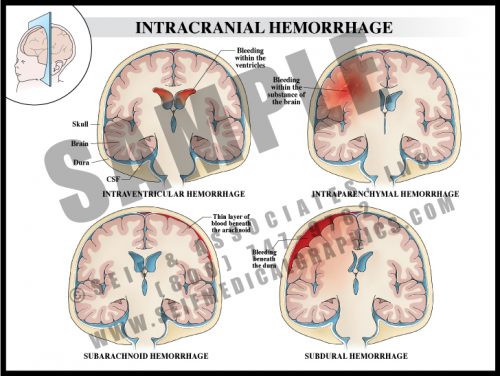
- Intraventricular hemorrhage is bleeding within the cavities of the brain that normally hold clear cerebrospinal fluid (CSF). Such bleeding is frequently associated with pre-term delivery and can result in hydrocephalus and loss of brain tissue.
- Intraparenchymal bleeding is within the brain tissue itself and usually results from ruptured arteriovenous malformation (AVM), hemorrhage following ischemic infarction or hypertension.
- Subarachnoid hemorrhage usually results from a ruptured surface AVM or cerebral artery aneurysm.
- Subdural hemorrhage is the result of trauma leading to disruption of bridging veins between the dura and the brain.
-
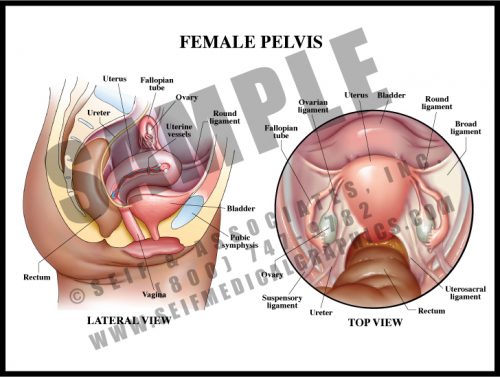
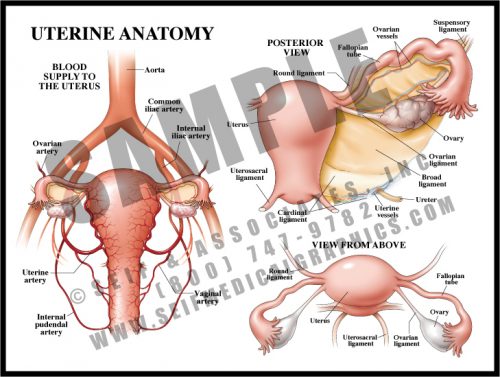
- The female pelvis contains the bladder, uterus, vagina, and rectum. The tissue between the vaginal and rectal openings is a tight collection of tendons from the pelvic floor muscles, the perineum. The entire region is called the vulva.
- The non-pregnant uterus is about the size of a small pear. It is a hollow muscular organ, its neck enclosed by a thick circular muscle known as the cervix.
- Urine is excreted from the kidneys via the ureters, which transport it to the bladder. It is then carried to the outside by the relatively short urethra.
- The ovaries release ova (eggs) each month to the uterus via the fallopian tubes; ovarian hormones are absorbed into the bloodstream.
- The organs are held in the pelvis by a number of ligaments connecting them to the pelvic walls.
-
- The uterus is small and contracted in its non-pregnant state, but grows to fill nearly the entire abdomen during pregnancy. Delivery is effected by repeated strong contractions pushing the fetus through the cervix and out the birth canal (vagina).
- The fallopian tubes carry the ova to the uterine cavity, where fertilized eggs implant and develop.
- The blood supply to the uterus is redundant and increases greatly during pregnancy.
-
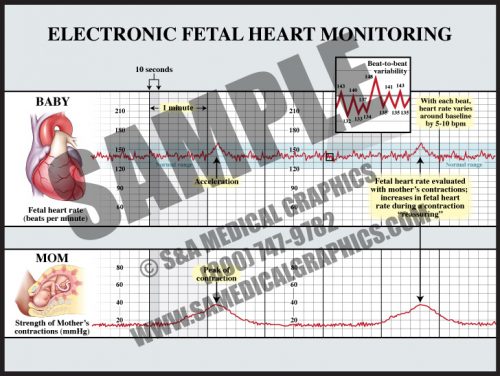
- This technology, used in approximately 87% of all labors in the U.S., tracks the fetal heart function against uterine contractions.
- The normal fetal heart rate is approximately 120-160 beats per minute (bpm), although normal individual fetuses might be higher or lower than this range.
- Beat-to-beat variability is literally the changes of the fetal heart rate from beat to beat (short-term variability), and within 3-5 minute periods (long-term variability). Beat-to-beat variability decreases or disappears for 20-30 minute time periods as the fetus sleeps, but is present in most normal labors and represents the health of the fetal brainstem.
-
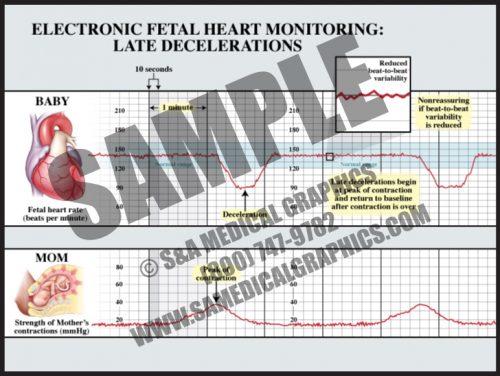
- Late decelerations start at or after the peak of a contraction and are considered to be a sign of uteroplacental insufficiency.
- The depth of late decelerations is probably not as significant as their presence. If frequent, they can be a sign of fetal distress and an indication for prompt delivery.
- If late decelerations are accompanied by loss of beat-to-beat variability, it is generally considered an indication for urgent or emergent delivery, either by cesarean section or operative delivery (forceps or vacuum extraction), depending upon the state of the labor.
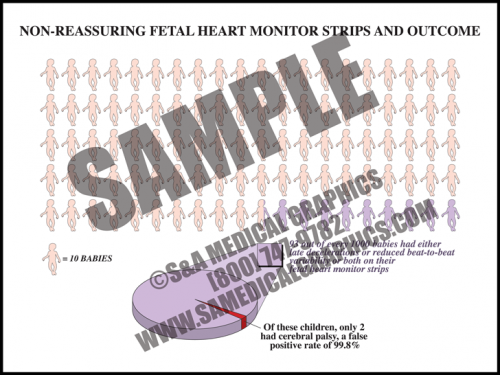
- The vast majority of fetuses with nonreassuring fetal heart tracings are completely normal.
-
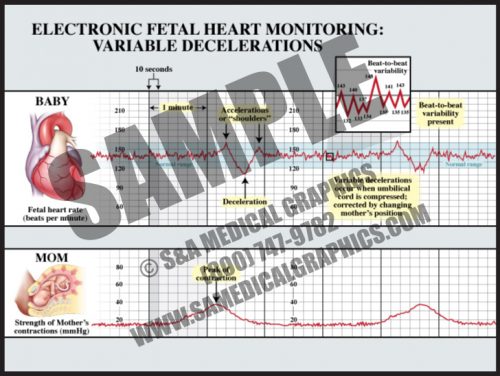
- Variable decelerations can occur at any time during or between contractions and are usually characterized by “shoulders” before and sometimes after the deceleration.
- The decelerations are usually “V” or “U”-shaped and return to baseline within two minutes or less.
- Variable decelerations are due to head or cord compression and are “treated” by changing the mother’s position and applying oxygen.
- Unless very deep (<60 bpm) for extended periods (>2 minutes or more), they are considered benign.
- Variable decelerations occur during the second stage of most labors, as the fetal head moves down the narrow vaginal canal and is compressed by a combination of the uterine contractions and the narrow vagina.
-
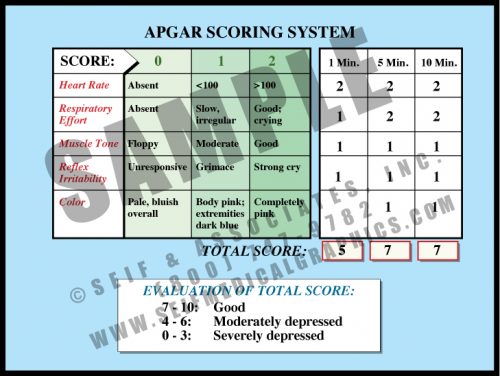
- This simple scoring system indicates how well the fetus fared through labor and delivery. The maximum score is 10 and the minimum is 0, with up to 2 points being awarded for each of 5 measures of health.
- Apgar scoring is done at 1 minute and 5 minutes of age, sometimes by nursing staff, sometimes by physicians. If the 5-minute score is low, a 10, 15 or 20-minute score may be recorded, either until the baby is stable or moved from the delivery room for specialized care.
- While there is some correlation between low 5 minute Apgar scores and neurological outcome, only a very small percentage of children with low 5 minute scores sustain brain damage. The longer the score remains low, the higher the correlation with neurological damage.
-
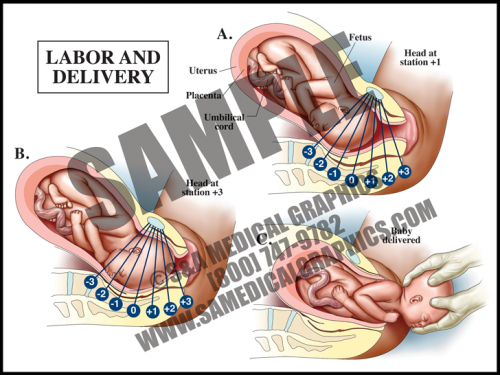
- In the first stage of labor, the cervix must thin (efface) and open (dilate) to a diameter of about 10 cm (4 in) in order to allow the fetal head to pass through.
- Repeated uterine contractions pushing the fetal presenting part against the inside of the uterus cause the cervix to thin and open over time.
- The fetal presenting part is considered to be engaged when the lowest portion is at the level of the ischial spines; this is called the 0 station. Fetal movement down the birth canal is measured by positive stations, using a 0/+3 scale or a 0/+5 scale.
- The second stage of labor starts at full dilation of the cervix and is completed when the fetus is delivered. The third stage is the delivery of the placenta.
-
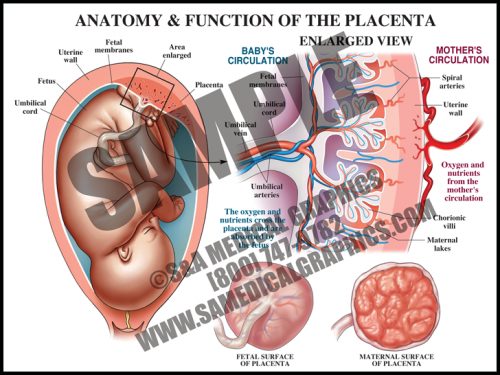
- The placental is a flattened, circular organ that develops in the uterus during pregnancy in order to support the fetus. The fetus is attached to the placenta via the umbilical cord.
- The placenta transfers oxygen and nutrients from the maternal blood to the fetal blood; it also transfers wastes products from the fetal blood to the maternal blood for removal.
- The umbilical cord is normally comprised of three blood vessels, two smaller umbilical arteries that carry deoxygenated blood from the fetus to the placenta, and a larger umbilical vein that supplies the fetus with oxygenated blood from the mother.
- The placenta is expelled from the uterus after the fetus is delivered. Placental pathology can reveal important information about intrauterine conditions and events, as well as shed light on the cause of adverse fetal outcome.
-
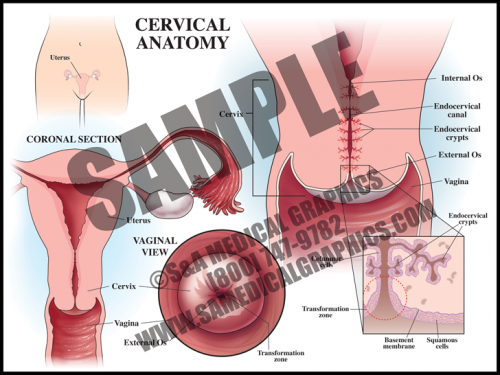
- The cervix is the circular muscle at the base of the uterus; it makes up the top of the vagina.
- The cervical canal passes through the cervix and allows blood from menstruation and a fetus to pass from the uterus into the vagina.
- During a pap smear, a screening test for cervical cancer, cells are scraped from the opening of the cervix and examined under a microscope for abnormality.
- The transformation zone is the area where the mucus secreting columnar cells of the endocervix meet the squamous cells of the ectocervix. Most squamous cell carcinomas and dysplasias are found here.
-
- One risk of fetal heart monitoring technology is false-positive results.
- In fact, “nonreassuring” FHM strips, or those which show either late decelerations, or reduced beat-to-beat variability, or both, have a greater than 99% false-positive rate in predicting cerebral palsy.
-
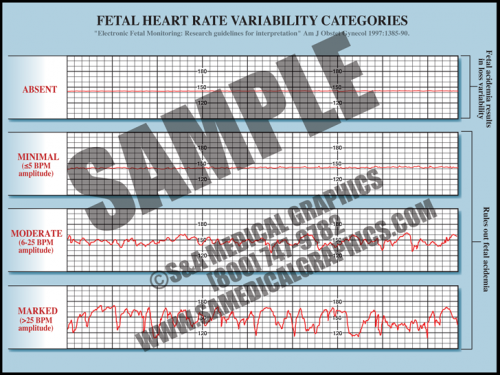
- Fetal heart rate is constantly varying from the baseline; this variability reflects a healthy fetal nervous system and cardiac responsiveness.
- These fluctuations are characterized as absent if there is no variation in the amplitude range, minimal if fluctuation is less than 5 bpm, moderate if fluctuation is 6 to 25 bpm, and marked if fluctuation is greater than 25 bpm.
- Absent variability indicates fetal academia but marked, moderate, and even minimal variation rules it out.
- Conditions like fetal hypoxia, congenital heart anomalies, and fetal tachycardia can cause a decrease in variability.
-
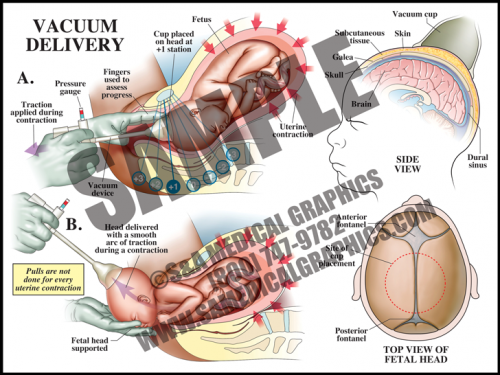
- Vacuum delivery may be performed in cases where there is a prolonged second stage of labor or suspicion of immediate or potential fetal compromise. This procedure assists delivery by helping to move the baby through the birth canal.
- The vacuum cap is a simple device that is placed on the vertex of the head with a small hand-held vacuum pump; some physicians leave the vacuum on between contractions and some release the vacuum. The caps are set to pop off if the vacuum pressure is too high.
- This procedure works with the uterine contractions, gently assisting and guiding the fetus out during contractions, and resting between them. It is not used between contractions.
-
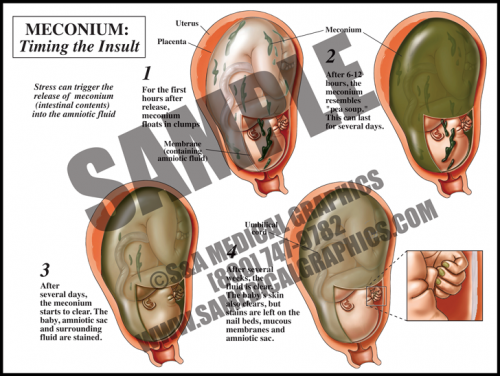
- Meconium is the dark, tarry contents of the fetal gastrointestinal tract. Meconium passage at labor and delivery is common and not a sign of fetal distress unless it is accompanied by other ominous signs.
- Meconium release into the amniotic fluid is however considered a sign of intrauterine fetal distress. This can be caused by placental insufficiency, maternal hypertension, and preeclampsia, among other things.
- When meconium is freshly released, it is clumpy and oats in the amniotic fluid. Within hours, it distributes particulate matter throughout the sac. Macrophages in the fetal skin, mucus membranes, and the amniotic sac phagocytize the particles, giving a green cast to the tissues.
- After several days, the fluid is greenish-brown but clear, and the fetus and membranes are stained. After several weeks, the fetal skin and fluid will clear, but the amniotic membranes, fetal mucus membranes, and nail beds remain stained.
-
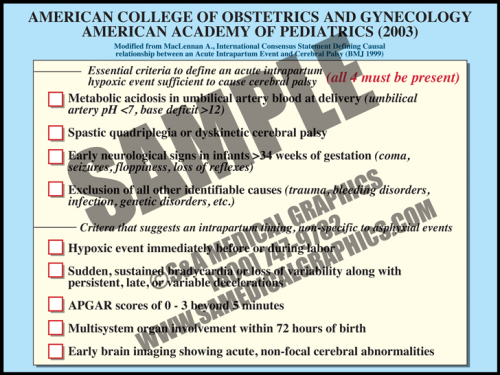
- In 2003, the American College of Obstetrics and Gynecology and the American Academy of Pediatrics recommended adoption of a definition of term intrapartum asphyxia developed by an international task force.
- The definition requires that all four parameters must be met in order to diagnose intrapartum asphyxiation in a term fetus. These include metabolic acidosis, diagnosis of specific types of cerebral palsy correlated with the types of asphyxia damage seen in term fetal brains, early seizures and other neurological signs, and exclusion of all other causes.
- There are other criteria that suggest an intrapartum timing of injury, nonspecific to asphyxia event. These include a hypoxic event immediately before or during birth, sudden, sustained bradycardia or loss of variability along with persistent, late, or variable decelerations, low APGAR scores (<3) beyond 5 minutes, multisystem organ involvement within 72 hours of birth, and early brain imaging showing acute, non-focal cerebral abnormalities.
-
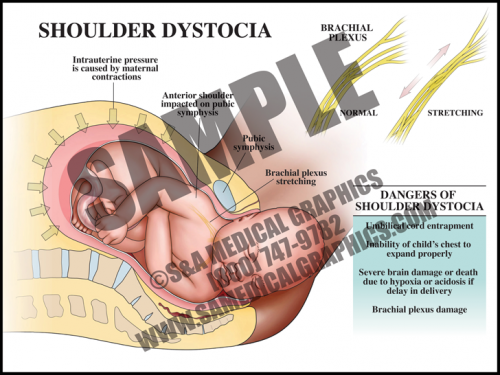
- In cases of shoulder dystocia, the upper fetal shoulder is impacted on the pubic symphysis, or more rarely, the lower shoulder becomes impacted on the sacral promontory or nonexible coccyx. In either case, this event prevents delivery of the baby. Shoulder dystocia can be a potentially catastrophic event since the fetal thorax is still within the pelvis and cannot properly expand for breathing.
- While the rate of shoulder dystocia is higher with gestational diabetic women and macrosomic fetuses (>4500 grams at birth), most cases of shoulder dystocia occur with average-sized fetuses.
- If a brachial plexus palsy (brachioplexopathy) occurs, it usually affects the portions of the brachial plexus that control the shoulder and elbow. Spontaneous recovery is the rule rather than the exception.
- Most fetuses are successfully delivered with a combination of McRoberts maneuver and suprapubic pressure.
-
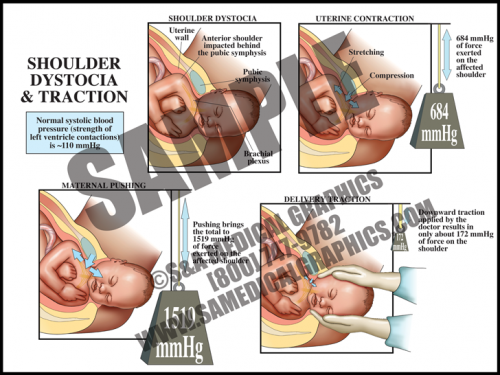
- The uterus itself generates tremendous pressure during contractions. If the average systolic blood pressure (pressure generated by the left ventricle during a contraction) is 120 mmHg, the uterus alone generates more than 5 times that amount. When the accessory muscles (the diaphragm and abdominal muscles) are used to push in conjunction with contractions, this pressure increases to more than 10 times that amount.
- The pull generated by a physician during downward traction for shoulder dystocia is slightly higher than the average systolic blood pressure and contributes only a very small amount to the total amount of generated pressures.
- Uterine and abdominal pressures are good evidence that if shoulder dystocia is the cause of brachial plexus palsy, it is most likely from the intrinsic pressures of the uterus and body wall, not the caregiver.
-
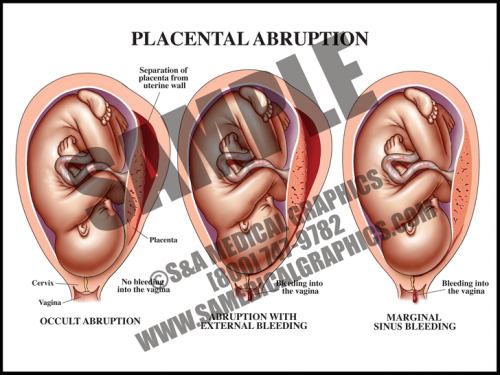
- Abruption occurs when the placenta separates from the uterine wall. Most of the time, this is accompanied by vaginal bleeding as the blood travels between the membranes and the uterus. Some- times, however, there is no bleeding because edges of the placenta remain sealed.
- Symptoms frequently include hypertonic uterus with severe abdominal pain and rapid contractions. If the abruption is large (more than about 50%), the fetus may not survive.
- The specific cause of placental abruption is often unknown, but risk factors include abdominal trauma and maternal factors like smoking, drinking, and diabetes, among others.
- Fetal distress occurs early in this condition in about half of all cases.
-
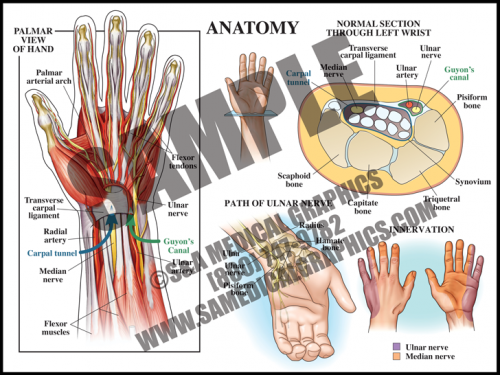
- The carpal tunnel is a passageway on the palmar side of the wrist that houses the median nerve and finger flexor tendons. Anteriorly, the carpal tunnel is bordered by the transverse carpal ligament, a heavy band of fibers that forms the fibrous sheath containing the carpal tunnel; posteriorly, the carpal tunnel is bordered by carpal bones.
- Guyon’s canal contains the ulnar nerve and artery; this anatomy does not pass through the tunnel, but lies superficial to it.
- Carpal tunnel syndrome occurs when the median nerve, which controls sensations to the palm side of the thumb, first, second, and half of the third finger, becomes compressed at the wrist, within the carpal tunnel. This results in pain, weakness, or numbness in the hand and wrist, radiating up to the arm.