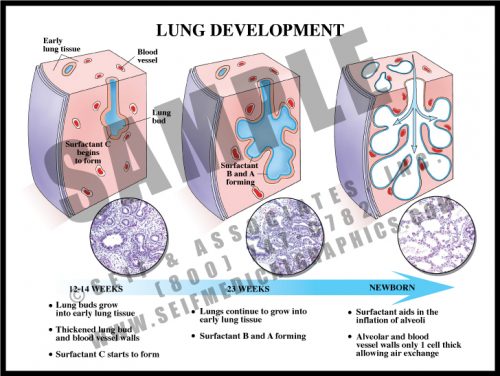
- The main reason that preterm infants are considered high risk is because their lungs are immature.
- Lungs develop as the airways bud and branch into an anlage of mesenchymal cells. Since respiration requires oxygen and carbon dioxide to cross over two layers of tissue (alveolar wall and capillary wall), these relatively thick-walled airways in preterm babies permit little gas exchange. High-pressure ventilation is required to assist the infant, and this pressure frequently results in the development of chronic lung disease (bronchopulmonary dysplasia).
- In addition, there are too few alveoli present for efficient oxygen supply until 2-3 weeks prior to term. Lungs continue to grow and develop new alveoli for several years after birth.
-
-
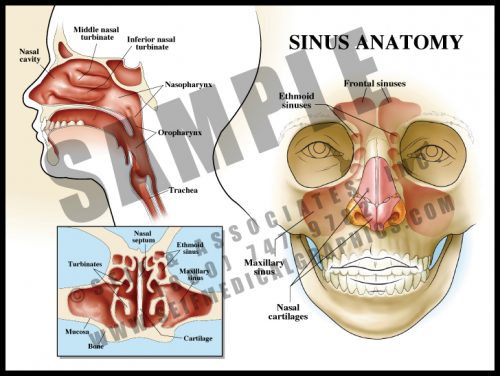
- Sinuses are hollow spaces within the facial bones. They are lined with a ciliated mucosa which has mucus glands. The sinuses are interconnected via a series of openings, allowing mucus to drain into the nose and pharynx.
- The sinuses help to warm inhaled air before it enters the lungs.
- Sinuses are prone to infection or reaction to allergens and react by mucosal swelling and overproduction of mucus. Chronic inflammation or infection can result in permanent thickening of the mucosa and reactive bone changes. Surgery is designed to facilitate drainage and relieve pressure; in some patients it must be repeated a large number of times.
-
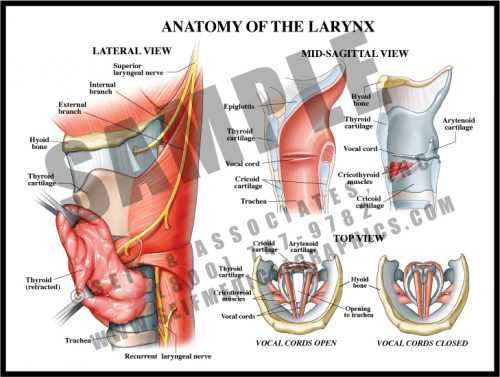
- The larynx is composed of a number of cartilaginous structures, muscles and ligaments which maintain the patency of the airway and hold the vocal cords under tension during speech.
- The large thyroid cartilage, which lies beneath the thyroid gland, is connected to the hyoid bone by a strong ligament (thyrohyoid ligament), and the epiglottis arises from its internal surface. All internal structures with the exception of the vocal cords are covered by a pink mucosal lining.
- The small cartilages to which the vocal cords are attached are moved by tiny muscles under the control of the recurrent, superior and inferior laryngeal nerves. These muscles make small adjustments in the opening between the cords, allowing different pitches of sound to be created.
-
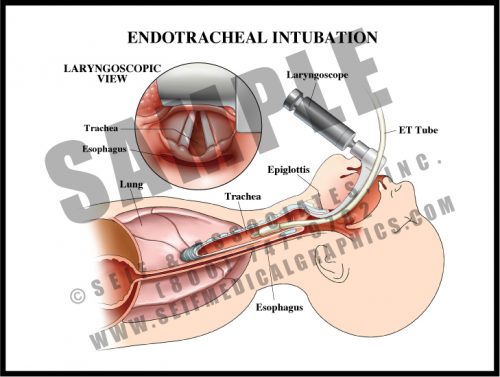
- Intubation is required when a patient has difficulty breathing and needs ventilatory assistance. A hollow tube is inserted into the trachea and held in place by a small inflated balloon. If intubation is required for more than a few weeks, a tracheostomy is used to replace it.
- Most endotracheal intubations are done using a laryngoscope, which holds the tongue and epiglottis out of the way while the health care provider inserts the ETT (endotracheal tube).
- Following ETT placement, the provider listens for bilateral breath sounds, watches for the chest to rise, and usually orders a portable chest x-ray to check ETT placement.
-
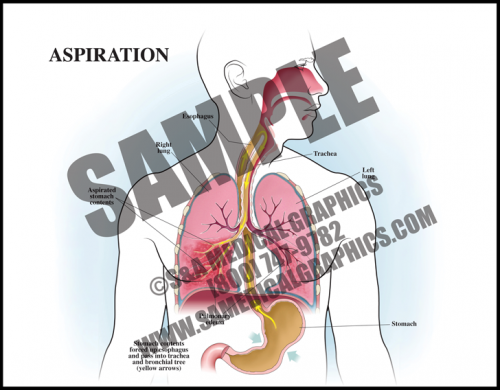
- Aspiration occurs when foreign material, of either oropharyngeal or gastric contents, is inhaled into the lungs.
- Aspiration can cause a number of respiratory problems depending on the quantity and nature of the inhaled material. Aspiration of gastric contents causes pulmonary edema and often pneumonia.
- The risk of aspiration is increased by conditions associated with altered or reduced consciousness, esophageal conditions like dysphasia, certain neurological disorders, and mechanical conditions like NG tube placement, endotracheal intubation, etc.
-
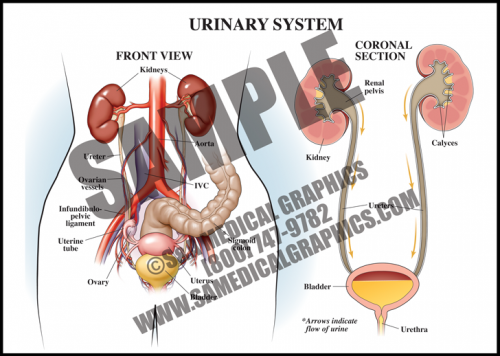
- The urinary system consists of the kidneys, ureters, bladder, and urethra. This system is responsible for removing wastes and extra fluid from the body in the form of urine. It also keeps the levels of electrolytes in the body stable.
- The kidneys filter the blood through specialized capillaries in order to remove waste materials and produce urine.
- The ureters drain urine from the kidneys and transport it to the bladder, where it is stored until it is released outside the body through the urethra during urination.
-
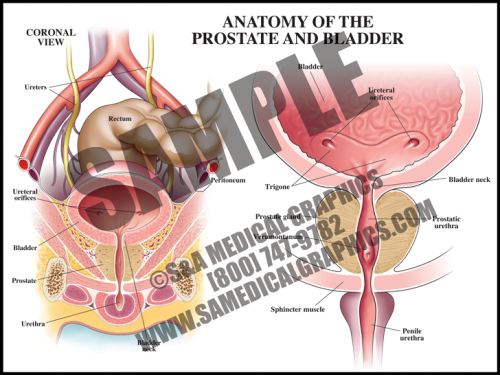
- The prostate is a walnut-sized gland located between the bladder and the penis; it secretes fluid that nourishes and protects sperm. The male urethra runs through the center of the prostate, from bladder to penis.
- The bladder is a hollow, muscular organ in the lower abdomen that stores urine and allows urination to be infrequent and voluntary.
- It is not uncommon for older men to develop benign prostatic hyperplasia (BPH), in which the prostate becomes enlarged, resulting in restriction of the ow of urine through the urethra. The prostate can also develop cancer, although that is much less common than BPH.
-
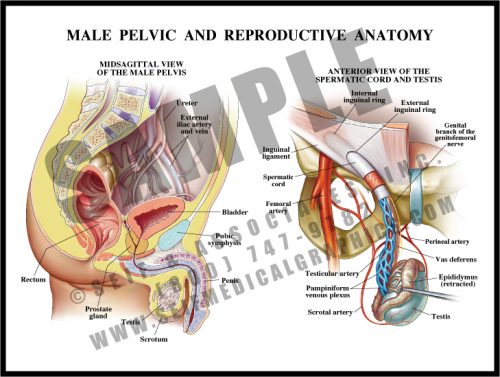
- The male pelvis contains the bladder and rectum, along with the internal portions of the reproductive system: the prostate, seminal vesicles, and the intrapelvic portions of the ductal apparatus.
- Sperm is produced in the testes, which lie in the scrotal sac outside of the pelvis. The sperm travels up the spermatic duct and is stored in the seminal vesicles. At ejaculation, sperm is released along with prostatic fluid, both of which travel down the urethra.
- The urethra has three parts: the prostatic portion; the membranous portion which passes through the urogenital diaphragm, and the penile portion.
- The spermatic cord contains a venous plexus, the spermatic artery and the spermatic duct.
-
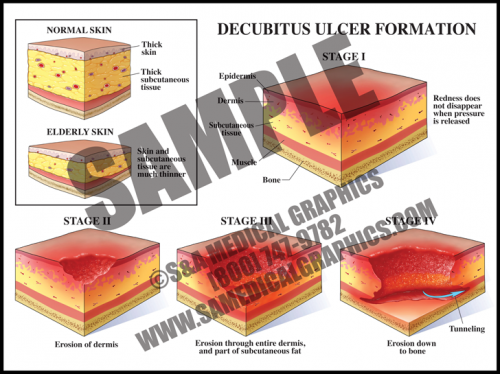
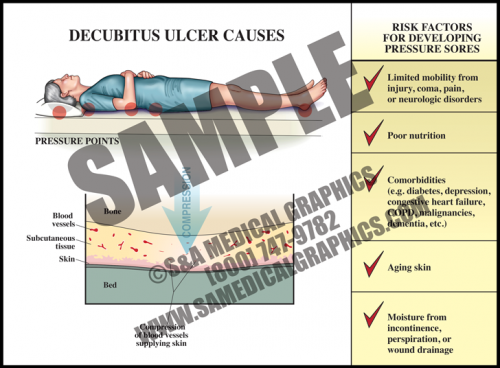
- Pressure ulcers are a localized injury to the skin and/or underlying tissue, usually over a bony prominence, that occur as a result of pressure, shear, and/or friction.
- Stage I decubitus ulcers manifest as a non-blanchable area of skin redness, which then progresses to a partial thickness wound in Stage II, and further to full thickness skin loss in Stage III. Stage IV decubiti involve full thickness tissue loss with exposed bone, tendon, or muscle with sloughing, undermining, and tunneling. These ulcers can extend into muscle and/or supporting structures making osteomyelitis and sepsis a concern.
- Decubitus ulcers are associated with an increased morbidity and mortality, and healing can be difficult as debilitated patients who form them usually have widespread vascular disease, nutritional de cits, and/or oxygenation/perfusion difficulties.
-
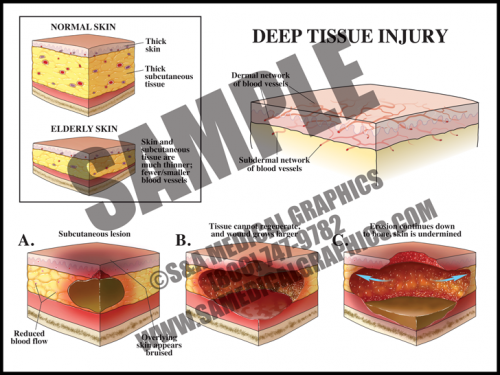
- Deep tissue injuries can have the same outward appearance as decubitus ulcers, but the underlying etiology is different. These injuries happen and progress quickly.
- The mechanism of this injury is pressure to the skin and soft tissue, within a short period of time, that compromises tissue perfusion and results in ischemia and damage to the deeper subcutaneous tissues.
- The initial injury is not visible on the surface of the skin and only manifests later as the underlying tissue starts to necrose, first forming what appears to be a bruise before progressing to an external/visible skin wound.
- This type of wound evolves upward towards the skin as well as deeper, so once the external wound becomes apparent, it is frequently already a deep injury often with the appearance of a Stage 3–4 decubitus ulcer.
-
- Decubitus ulcers are common in debilitated patients, particularly the aged who have thinner skin and subcutaneous tissue that is more susceptible to compression injury.
- Patients with limited mobility (from injury, sickness, or neurologic disorders, etc.), poor nutritional intake, conditions affecting perfusion and oxygenation of tissues (like diabetes, cardiovascular disease, heart failure, etc.), skin moisture due to incontinence, and advanced age are particularly vulnerable.
- These ulcers are often multifactorial, making them difficult to prevent and even more difficult to heal in at-risk patients.
-
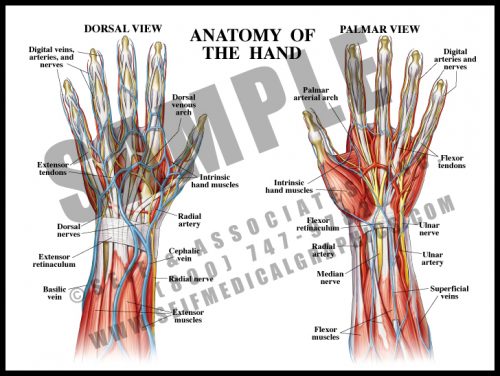
- One of the more complex structures, the hand has a high concentration of nerves and vessels. There are also many small intrinsic muscles which allow fine motor function.
- Tendons, blood vessels and nerves originating in the arm cross the wrist to enter the hand; the intrinsic muscles are solely within the hand.
- The structures crossing the double row of wrist bones are held in place by the flexor retinaculum on the volar (palmar) side (“carpal tunnel”), and by the extensor retinaculum on the dorsal side. The flexor retinaculum can sometimes thicken or scar, causing compression of the median nerve, or carpal tunnel syndrome.
-
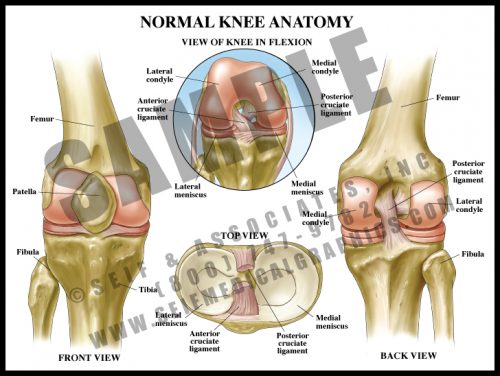
- One of the major joints in the body, the knee is required to support huge and repeated pressures over the course of a lifetime. The articular surfaces of the joint are covered with glassy-smooth articular cartilage, and the menisci act as shock absorbers with each step.
- The patella is a large sesamoid bone which lies within the quadriceps tendon. It articulates with the condyles of the femur.
- The anterior and posterior cruciate ligaments are located at the center of the joint and allow some rotatory motion. The lateral and medial collateral ligaments are attached on either side of the joint to maintain stability.
-
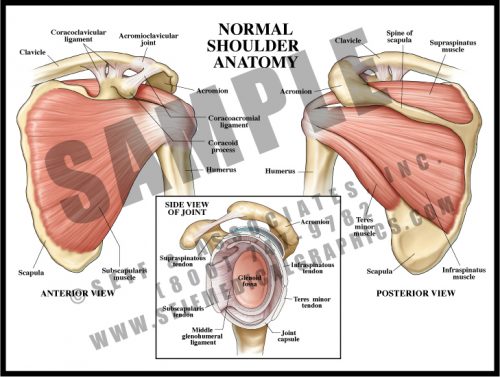
- The tendons of the deep shoulder muscles (infraspinatus, supraspinatus, and teres minor) conjoin with the shoulder joint capsule to form the rotator cuff.
- Rotator cuff injuries are common and may be difficult to treat.
- The head of the humerus rests in the glenoid fossa, a relatively shallow depression in the scapula. The rotator cuff holds the head in the fossa during movement.
- The shoulder joint is prone to dislocation due to the shallowness of the glenoid fossa.
- The acromioclavicular joint lies over the shoulder and sometimes develops fibrosis, making movement painful or stiff.
-
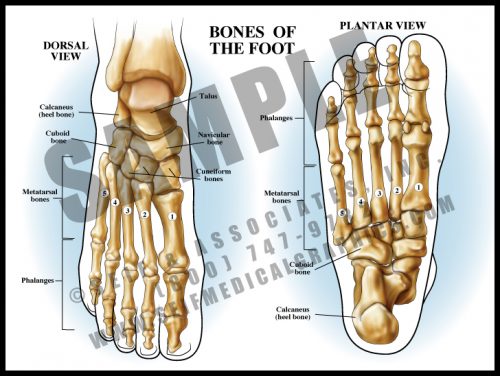
- The bones of the foot follow basically the same pattern of the hand bones. There is a double layer of sesamoid-like bones forming the ankle, which articulate with the long bones making up the central foot (metatarsals), which are in turn attached to the phalanges, or toes.
- The tendons and the many ligaments of the foot attach to the tough, thin tissue covering the bones, the periosteum. The ligaments attach the bones to each other, and the tendons connect the muscles to the bones.
- As in the hand, there are intrinsic muscles in the feet.
- The bones of the foot form a longitudinal arch and a transverse arch. Most of the body’s weight is borne on the metatarsal heads, particularly the first and fifth.
-
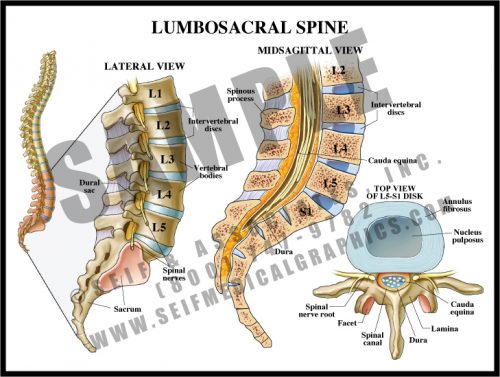
- The lumbar spine is composed of large, strong bones which must support the entire weight of the spine and head.
- The vertebral bodies are separated by fibrous discs which serve as shock absorbers. The discs have a fibrous ring (annulus fibrosis) and a gel-like center (nucleus pulposus).
- The spinal canal is formed by the pedicles, laminae, and the vertebral bodies and discs; the canal protects the distal portion of the axial nervous system, the cauda equina.
- The large transverse and spinous processes serve as support for the many paraspinous muscles which allow for the fine movement of the spine.
- The sacrum is the large, wedge-shaped bone forming the posterior part of the pelvic bowl, and is composed of fused vertebrae.
-
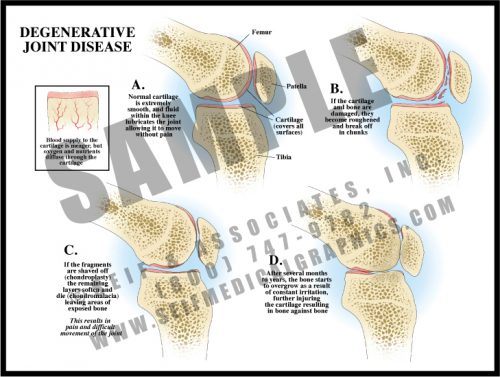
- Degenerative joint disease is a result of normal activity and is found in most people as they get older; it develops more rapidly and more severely in the case of joint trauma.
- Articular surfaces are covered with glassy-smooth cartilage. As the cartilage disintegrates over time (chondromalacia), it flakes off until the bone is eventually exposed.
- If bone starts to rub against bone, it reacts by forming more bone in the form of osteophytes. This is a very painful condition and when severe enough, requires joint replacement.
- Degenerative joint disease is frequently called osteoarthritis; rheumatoid arthritis is an autoimmune disease with very different causes and a slightly different set of symptoms.
-
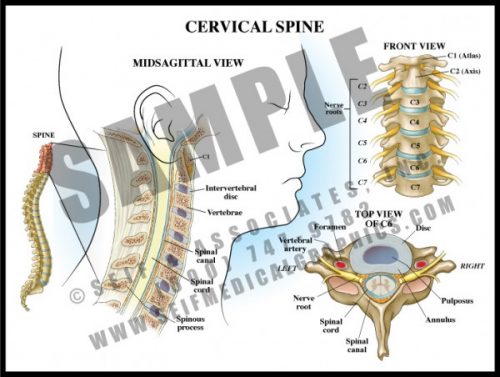
- The 7 vertebrae of the cervical spine help support the skull and protect the spinal cord as it exits the cranium to pass downward through the spinal canal.
- The transverse processes each have a small hole through which the vertebral arteries pass to join to form the basilar artery supplying the posterior and deep portions of the brain and brainstem.
- The cervical nerve roots form the brachial plexus which supplies sensation and movement to the upper extremities.
- Degenerative joint disease and disc disease are very common in the cervical spine, leading to arm and hand pain and dysfunction requiring decompression and sometimes fusion.
-
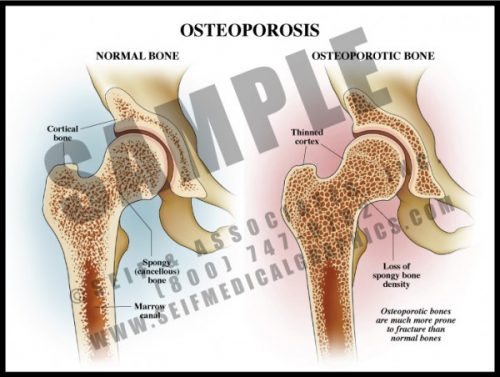
- A common condition, particularly among elderly women, osteoporosis is the reduction of bone density.
- Osteoporosis affects both the dense cortical portion on the outside of a bone and the spongy bone inside.
- Causes include age, low body mass, family history, smoking, malnutrition, alcoholism, insufficient physical activity and certain medications and toxins. It is also associated with a number of chronic diseases.
- The primary risk is that of fracture, particularly of the hip, a potentially devastating event in the elderly. In severely osteoporotic patients, healing may be slow and insufficient.
- Treatment depends on the cause but includes medication, dietary changes, and exercise.
-
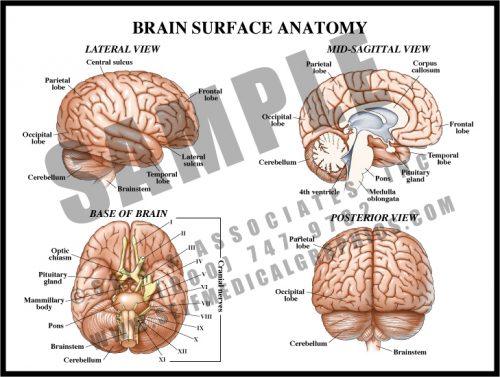
- The surface of the brain has multiple folds, or gyri, separated by sulci. While many of these are specific to a particular individual, some are constant and serve as landmarks for functional control.
- The cerebrum is the large, rounded portion of the brain and is the site of higher functions. The cerebellum and brainstem control more basic functions like heart rate, balance, and respiration.
- The cranial nerves mostly originate in the brainstem and exit the skull via foramina in the base of the skull (see M1). The optic nerves originate in the occipital lobes, travel along pathways inside the brain matter, and exit anteriorly.
- The corpus callosum is a group of myelin-covered neuronal fibers (white matter) which connect the right side of the brain with the left.
-
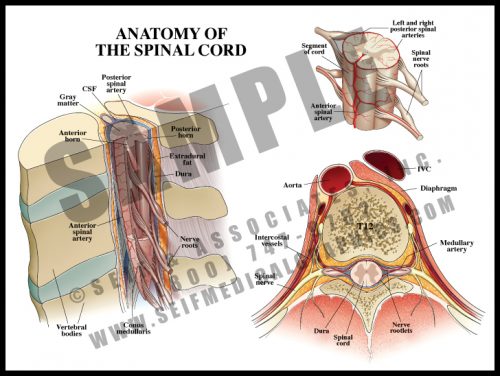
- The spinal cord lies within the spinal canal, formed by the vertebral bodies and the bony arch formed by the pedicles and laminae (see M6).
- The cord and its terminal nerves, the cauda equina, lie within the dural sac, a tough membranous structure filled with cerebrospinal fluid bathing and protecting the cord.
- The spinal cord itself ends at the level of the first lumbar vertebra, but nerve roots travel inside the dural sac to exit at lower levels; these roots form the cauda equina (”horse’s tail”).
- Blood supply comes from the segmental branches of the aorta, traveling along the nerve root to emerge as the anterior spinal artery running in the front midline of the cord; there are two parallel vessels along the back surface of the cord. There is also a generous venous plexus within the canal.
-
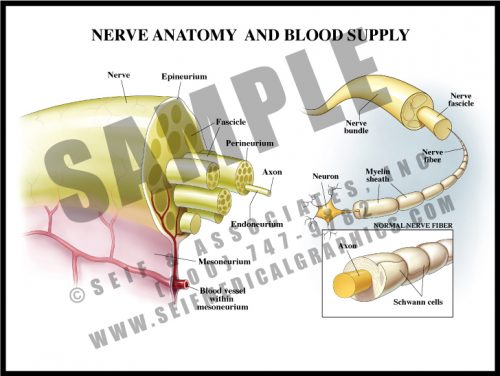
- Nerves are composed of multiple fibers which in turn are composed of many, many axons. Each successive grouping of fibers is surrounded by connective tissue.
- Axons are the long branches of nerves cells which transmit electrochemical impulses from one nerve to another or to and from target organs.
- The axons are surrounded by myelin, a kind of insulating material formed by oligodendrocytes. In diseases in which myelin is destroyed, electrochemical conduction is impossible, and even if the nerve fibers do not die, they are ineffective.
- Blood vessels travel through the mesoneurium and then divide into capillaries within the nerve to deliver oxygen and nutrients.
- Nerves are vulnerable to trauma, reduced oxygen levels, and diabetes.
-
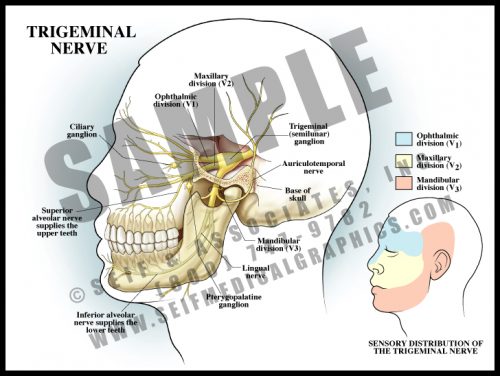
- The semilunar ganglion of the trigeminal nerve lies deep within the skull. The three branches of the nerve leave through large separate openings in the base of the skull.
- The trigeminal nerve is the 5th cranial nerve. Its three portions are the ophthalmic nerve controlling sensation to the upper face, the maxillary nerve controlling sensation to the mid-face, and the mandibular nerve supplying sensation to the lower face and the skin around and above the ear. Each of the branches supplies both soft tissue and bone.
- All large ganglia in the body can harbor certain viruses. Oral herpes infections “hibernate” within the semilunar ganglion, traveling down the nerve roots to the mouth when the virus is activated by stress.
-
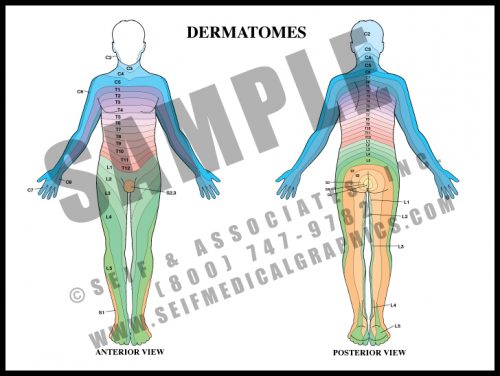
- Dermatomes are strips of skin which are supplied by the nerve roots. If there is numbness or pain along a dermatome, it is a sign of damage or irritation of a specific nerve root, where the root exits the spinal cord and vertebral column. This is known as radiculopathy.
- Soon after the cervical and lumbosacral nerves leave the cord, they join and separate several times (plexi) before reaching their target organs. Nerve fibers to a given muscle may come from several different nerve roots. The skin sensory supply, however, remains directly associated with the root alone.
- Radicular pain usually occurs with compression of the nerve in the foramen, the hole by which the nerve exits the spinal canal.
-
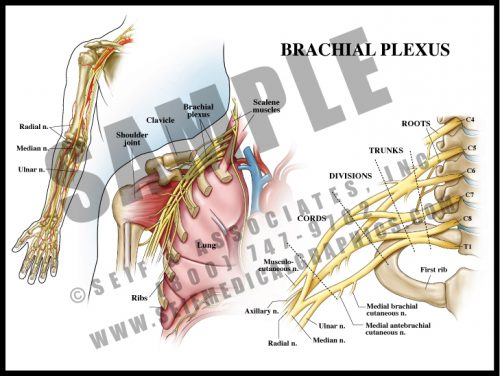
- The nerve roots of the lower cervical spinal cord split and merge several times before supplying the arm and hand.
- The brachial plexus lies over the first rib and behind the clavicle. It is intimately related to the subclavian/brachial artery and passes between the scalene muscles of the neck.
- The plexus is divided into roots, trunks, divisions, cords and terminal branches. By looking at the anatomical distribution of pain or dysfunction, it is possible to determine the location of a brachial plexus lesion.
- Brachial plexopathy can occur during delivery with or without shoulder dystocia, and from thoracic outlet syndrome.
-
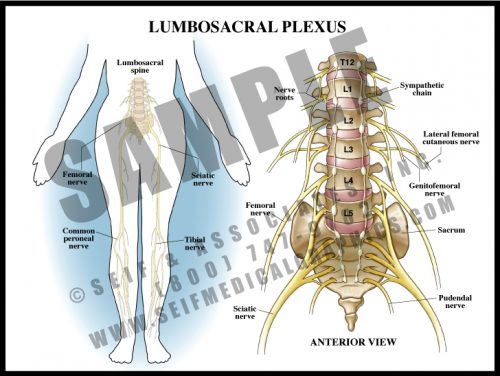
- Analogous to the brachial plexus, the lumbosacral plexus is a series of nerve convergences and separations which ultimately combine into several large terminal nerves.
- Plexi form a protective mechanism in that if one nerve root is damaged, a particular muscle might be weakened, but function would not be completely lost.
- The terminal nerves in the legs generally follow the course of the deep vasculature.
- Terminal sensory nerves to the feet are particularly vulnerable to diabetes, resulting in peripheral diabetic neuropathy. This frequently contributes to foot infections and the need for amputation.
-
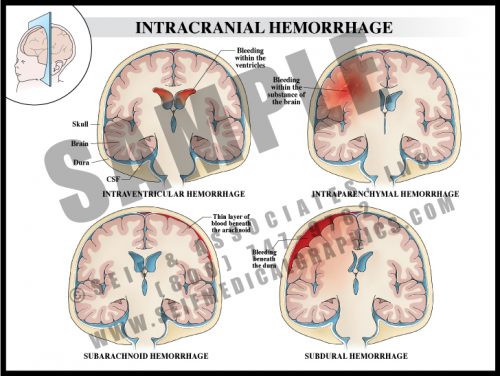
- Intraventricular hemorrhage is bleeding within the cavities of the brain that normally hold clear cerebrospinal fluid (CSF). Such bleeding is frequently associated with pre-term delivery and can result in hydrocephalus and loss of brain tissue.
- Intraparenchymal bleeding is within the brain tissue itself and usually results from ruptured arteriovenous malformation (AVM), hemorrhage following ischemic infarction or hypertension.
- Subarachnoid hemorrhage usually results from a ruptured surface AVM or cerebral artery aneurysm.
- Subdural hemorrhage is the result of trauma leading to disruption of bridging veins between the dura and the brain.
-
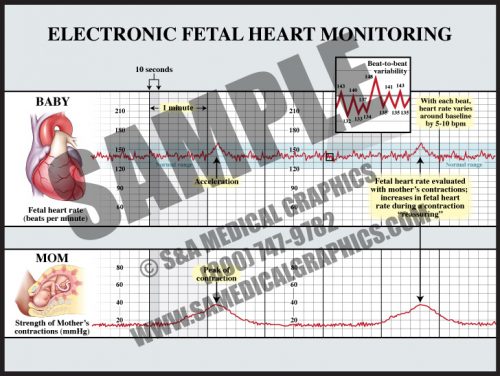
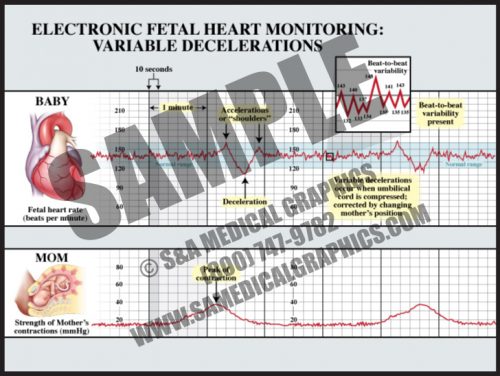
- This technology, used in approximately 87% of all labors in the U.S., tracks the fetal heart function against uterine contractions.
- The normal fetal heart rate is approximately 120-160 beats per minute (bpm), although normal individual fetuses might be higher or lower than this range.
- Beat-to-beat variability is literally the changes of the fetal heart rate from beat to beat (short-term variability), and within 3-5 minute periods (long-term variability). Beat-to-beat variability decreases or disappears for 20-30 minute time periods as the fetus sleeps, but is present in most normal labors and represents the health of the fetal brainstem.
-
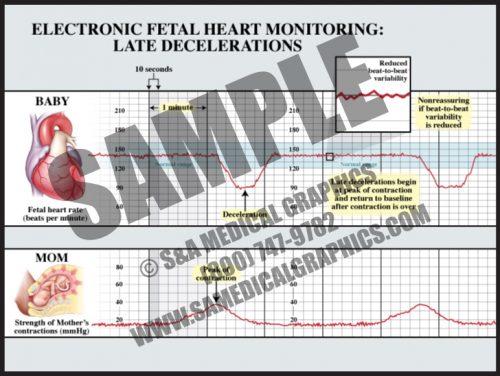
- Late decelerations start at or after the peak of a contraction and are considered to be a sign of uteroplacental insufficiency.
- The depth of late decelerations is probably not as significant as their presence. If frequent, they can be a sign of fetal distress and an indication for prompt delivery.
- If late decelerations are accompanied by loss of beat-to-beat variability, it is generally considered an indication for urgent or emergent delivery, either by cesarean section or operative delivery (forceps or vacuum extraction), depending upon the state of the labor.
- The vast majority of fetuses with nonreassuring fetal heart tracings are completely normal.
-
- Variable decelerations can occur at any time during or between contractions and are usually characterized by “shoulders” before and sometimes after the deceleration.
- The decelerations are usually “V” or “U”-shaped and return to baseline within two minutes or less.
- Variable decelerations are due to head or cord compression and are “treated” by changing the mother’s position and applying oxygen.
- Unless very deep (<60 bpm) for extended periods (>2 minutes or more), they are considered benign.
- Variable decelerations occur during the second stage of most labors, as the fetal head moves down the narrow vaginal canal and is compressed by a combination of the uterine contractions and the narrow vagina.