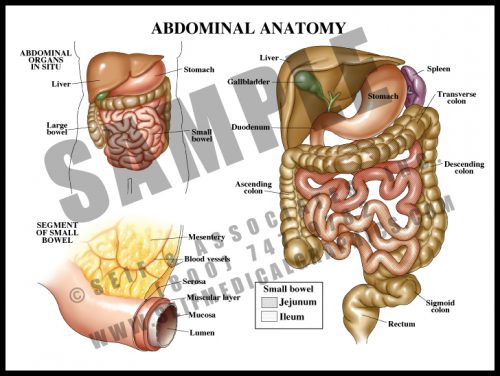
- The contents of the abdomen are primarily associated with digestion and distribution of nutrients.
- The esophagus, a tube which carries food and fluid through the thorax, enters the abdomen through the diaphragm, where it widens into the stomach; the stomach empties into the small bowel (duodenum, jejunum, and ileum, in which food is absorbed into the blood stream), and from there into the large bowel, where waste material is compacted as fluid is reabsorbed into the system.
- The liver has multiple functions affecting a number of other body systems, including digestive, hematologic and endocrine/metabolic.
- The large and small bowels are supplied by branches off of the aorta carried within the mesentery, a double-layered sheetlike structure.
-
-
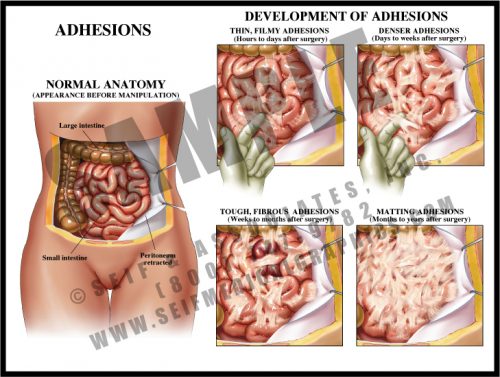
- Adhesions are fibrous scars which can form after any disturbance within body cavities and spaces. Inciting events can include surgery, trauma, and inflammation.
- Within hours of disturbance, thin, filmy strands form between bowel loops and between bowel and peritoneum and/or body wall. These continue to form for a period of time and mature over a period of weeks.
- Mature adhesions are dense, white fibrous tissues which have merged with the outer layer of the tissues; they eventually develop their own blood supply and may become severe enough to cause chronic pain and pose a chronic risk of small bowel obstruction or volvulus.
-
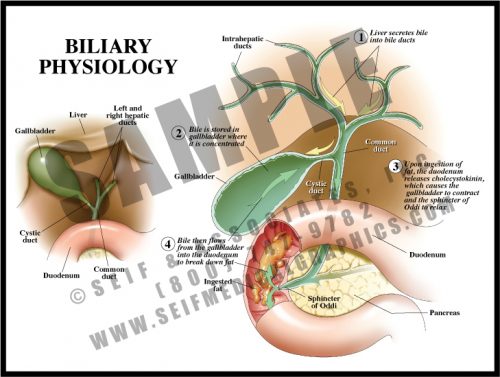
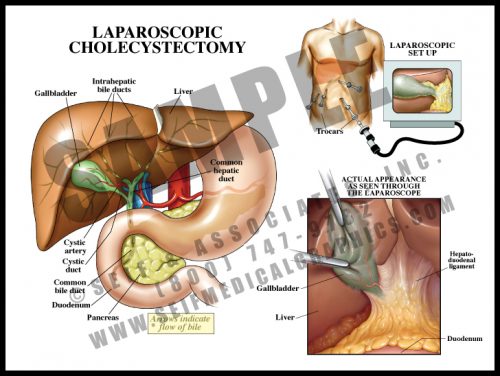
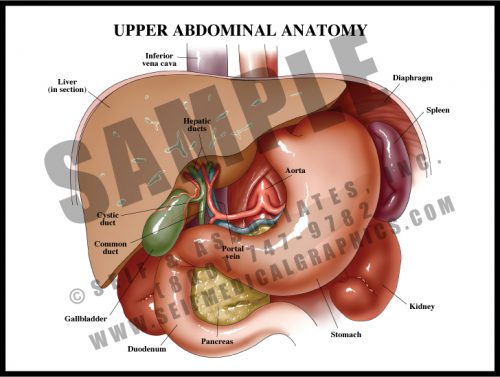
- The gallbladder stores bile formed within the liver, releasing it for fat digestion.
- Bile travels through the intrahepatic ducts into the paired hepatic ducts; these merge into the common hepatic duct. Bile is then diverted via the cystic duct to the gallbladder for storage.
- When food is ingested and travels through the stomach to the duodenum, a hormone is released (cholecystokinin) which stimulates the gallbladder to contract and the sphincter of Oddi to relax. This allows bile to flow through the cystic duct and the common bile duct into the duodenum.
- The most common pathology in the extrahepatic biliary system is bile (gall) stones (concretions of bile salts, cholesterol, and minerals) which can block ducts, causing inflammation, pain, and jaundice.
-
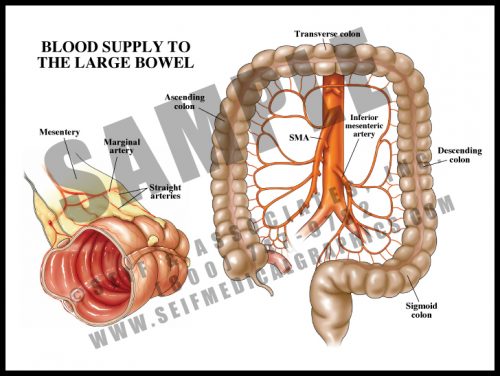
- The blood supply of the colon comes from three sources: the superior mesenteric arteries supplying the cecum, ascending (right) colon and half of the transverse colon; the inferior mesenteric arteries supplying the distal half of the transverse colon, the descending (left) colon, and the sigmoid colon; the rectal arteries supply the rectum.
- The arteries then divide into arcades, as they do to the small bowel, with straight arteries entering the bowel wall at the mesenteric border.
-
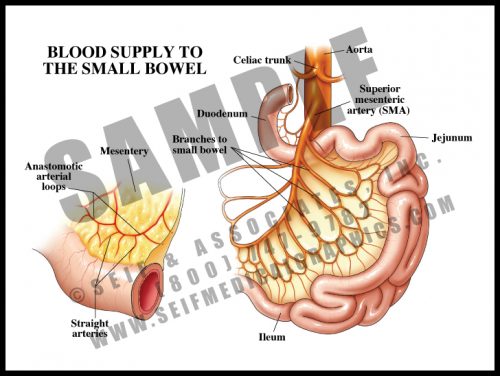
- With the exception of a portion of the first part of the duodenum, the small bowel is supplied by the many branches of the superior mesenteric artery.
- The branches anastomose with each other in two layers of arcades or arches, and from these, small straight vessels pass to the bowel surface, traveling around and through the wall, dividing into smaller and smaller branches.
- The arcades and multiple straight vessels are an adaptation which protects the bowel. Damage can occur to a portion of the small bowel without loss of the entire organ. Clots and ischemia from atherosclerosis and other vascular pathologies can affect the small bowel, much like the brain, heart, kidney and other organs can be affected by such conditions.
-
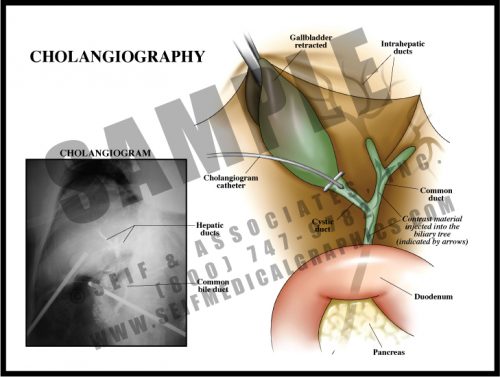
- Performed during surgery for gallbladder removal, this is an effective intraoperative radiographic test to look for either blockage or leakage in the biliary tree.
- This test may be performed prior to removing the gallbladder, or at any time a problem is suspected. A tiny catheter is threaded through a small incision in the cystic duct. Dye is injected into the biliary tract and x-rays are taken, allowing the surgeon to see which ducts are patent. Voids represent stones or tumors, and extravasation represents a leak in the system.
- While this test is very reliable in the case of a retained stone or suspected damage, the outcome in patients having routine intraoperative cholangiography without apparent complication is the same as those in whom the test was not performed.
-
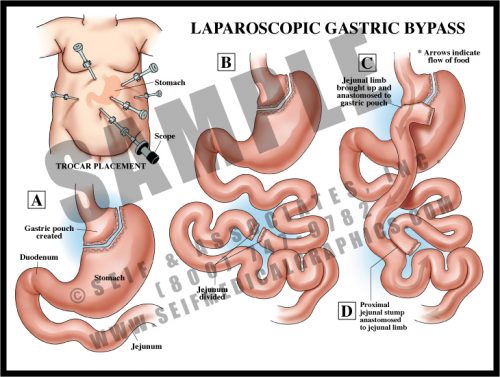
- Gastric bypass is performed to reduce the volume of food which the stomach can hold, and to reduce the amount of bowel available to absorb nutrients.
- There are several surgical variations; in this version, the stomach is divided and the small bowel is surgically joined to the small stomach remnant, bypassing the rest of the stomach. A second surgical anastomosis is made further down the length of the small bowel. No tissue is removed.
- The procedure can be performed either through a large abdominal incision or laparoscopically, using “band-aid” incisions. A lighted scope is inserted into the abdomen, as are several slender tubes. Instrumentation is then placed into the tubes and the procedure is performed under direct vision through the scope.
-
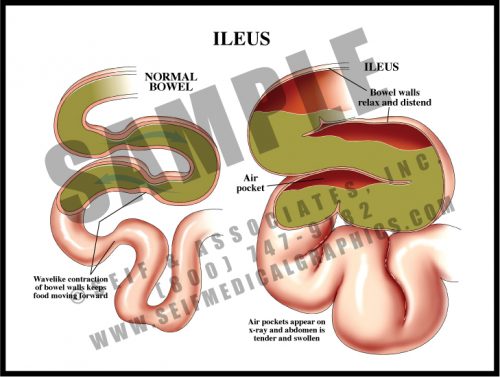
- Normal small bowel function is in the form of peristalsis, regular wave-like contractions of the smooth muscle within the wall of the bowel. Digested food materials (chyme) move through the small bowel, where intestinal villi absorb nutrients. These raw materials enter the bloodstream and are distributed throughout the body for growth and maintenance.
- Ileus is a temporary reduction or cessation of peristalsis, allowing fluid, chyme, and gases to accumulate. It is characterized by abdominal distension and discomfort; on x-ray, distended bowel loops with air/fluid levels can be seen. Bowel sounds are reduced or absent, and gas and stool are not passed.
- Ileus is a common sequela of abdominal or pelvic surgery, lasting hours to days. Symptoms are relieved by nasogastric suction to reduce pressure.
-
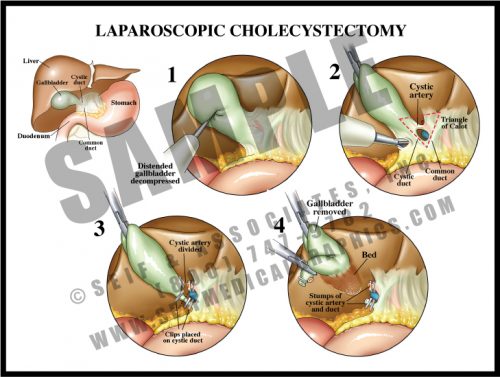
- After placement of the trocars, the gallbladder is grasped and retracted upward and outward. Adhesions, connective tissue, and the lesser omentum are divided from the neck of the gallbladder in a medial direction, to reveal a portion of the cystic duct.
- Clips are placed on the exposed cystic duct and an incision is made between the clips.
- The cystic artery is then located within the Triangle of Calot (formed by the planes of the lower border of the liver, the cystic duct, and the common hepatic duct), ligated and divided.
- The gallbladder is removed through one of the ports.
-
- Cholecystitis, or inflammation of the gallbladder, is usually caused by gallstones blocking the cystic duct. Removal is usually performed via a laparoscopic approach, using an endoscope for visualization and hollow trocars holding the small instruments used for the surgery.
- The view through the laparoscope is transmitted to a video monitor, and the physician controls the progress by either looking directly through the scope or at the video display, depending on his or her preference and training.
- The overall complication rate for the laparoscopic procedure is about half that of the open procedure, although converting a laparoscopic procedure to an open one occurs approximately 4% of the time, usually because of difficulty in visualization.
-
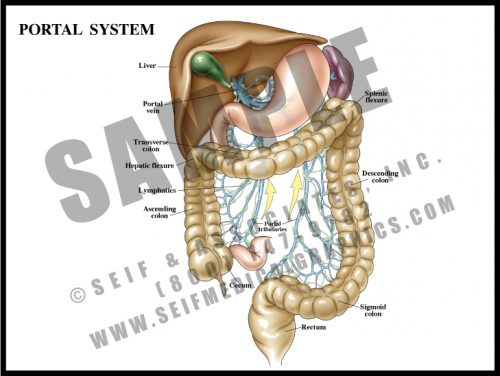
- The portal system is a specialized venous drainage system of the large bowel. Instead of merely draining deoxygenated blood, the portal system drains metabolites and nutrients upward so that they detour through the liver instead of returning directly to the heart and lungs. The liver serves as a cleaning and metabolic sieve where drugs and other chemicals are further broken down and either used or removed from the system.
-
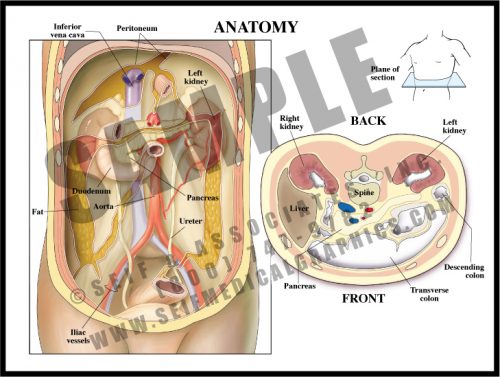
- Most of the abdominal contents lie within the peritoneum, a sac made up of a sheet of dense connective tissue. Some structures lie behind the peritoneum (retroperitoneal). Others go in and out of it, although edges are sealed and there is little or no direct connection between the intra- and retroperitoneal regions.
- The liver has a “bare area” at its top where it lies directly against the lower surface of the diaphragm, but the rest of it is intraperitoneal. The ascending and descending colons are both retroperitoneal, while the transverse colon and part of the sigmoid are intraperitoneal; the duodenum, or first portion of the small intestine, is retroperitoneal.
- True retroperitoneal structures include the pancreas, the kidneys, ureters and adrenals, the great vessels and the pelvic structures.
-
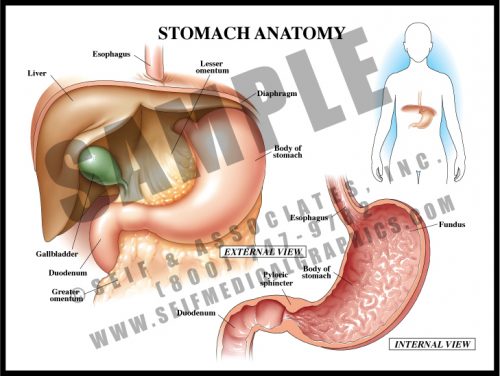
- The stomach is a muscular sac derived from the simple fetal gastrointestinal tube. The mucosal lining has specialized cells which secrete strong acids and enzymes to break food down before it passes to the small bowel for absorption and distribution.
- The walls are folded into rugae which increase the surface area of the sac. The muscular walls contract to help break up food material.
- The greater omentum arises from the greater curvature of the stomach, and the lesser omentum from the lesser curvature; the hepatoduodenal ligament lies at the free edge and contains the extrahepatic biliary ducts.
- The stomach lies under the diaphragm and to the left of the liver. The strong pyloric sphincter divides the distal stomach from the duodenum or the first portion of the small intestine.
-
- The primary function of the upper abdominal organs is the breakdown of food for distribution by the small bowel. Chewed and macerated food travels through the esophagus to the stomach, where strong acids and muscular contractions break it down further.
- Proteolytic enzymes from the pancreas and bile from the liver and gallbladder drain into the duodenum to further the digestion and breakdown of food.
- The spleen functions as part of the hematopoietic system, controlling the distribution and eventual destruction of red blood cells. It also acts as a part of the immune system.
- Blood is supplied to most of these structures by branches of the celiac trunk, the first major aortic branch in the abdomen.