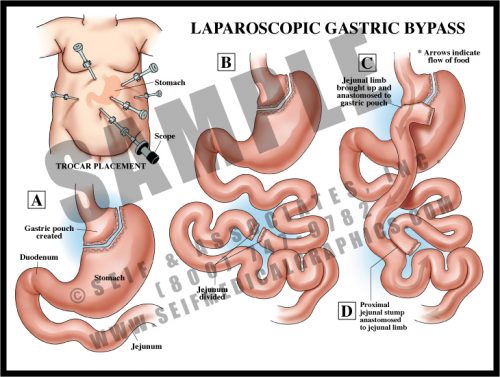
- Gastric bypass is performed to reduce the volume of food which the stomach can hold, and to reduce the amount of bowel available to absorb nutrients.
- There are several surgical variations; in this version, the stomach is divided and the small bowel is surgically joined to the small stomach remnant, bypassing the rest of the stomach. A second surgical anastomosis is made further down the length of the small bowel. No tissue is removed.
- The procedure can be performed either through a large abdominal incision or laparoscopically, using “band-aid” incisions. A lighted scope is inserted into the abdomen, as are several slender tubes. Instrumentation is then placed into the tubes and the procedure is performed under direct vision through the scope.