- This 2D animation demonstrates the nor- mal course of labor, showing the dilation of the cervix, descent of the fetus, delivery of the fetal head, and finally delivery of the fetal shoulders and body.
- This animation has pause and play buttons to allow for more interactivity during viewing.
-
-
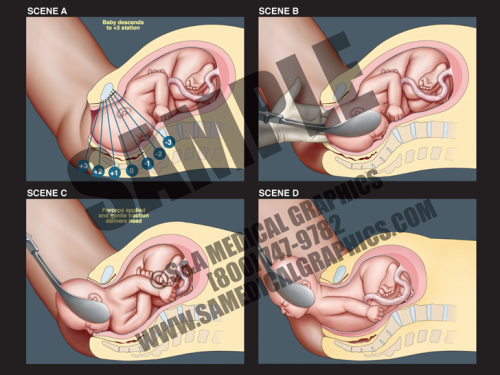
- Forceps delivery is a type of operative vaginal delivery performed to help guide the baby out of the birth canal if the second stage of labor isn’t progressing or if fetal safety depends on immediate delivery.
- This 2D animation shows how this procedure is performed, showing that once the fetus has descended far enough down the birth canal, a health care provider applies the forceps to the fetal head.
- The forceps are then used to gently assist and guide the fetus out of the birth canal during uterine contractions. Forceps are not used between contractions.
-
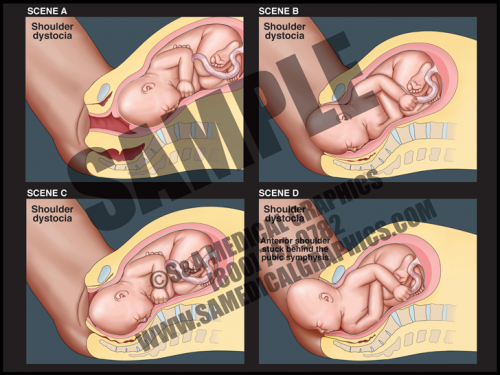
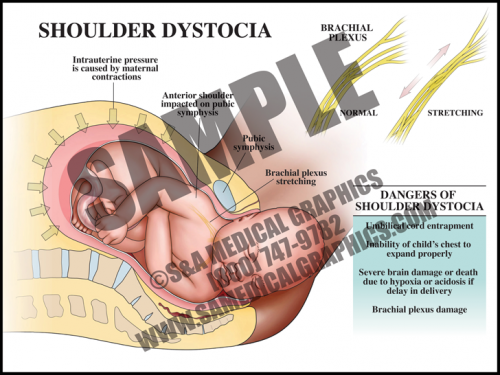
- This 2D animation demonstrates how shoulder dystocia occurs during delivery.
- It shows fetal descent down the birth canal and delivery of the fetal head, but impaction of the anterior shoulder on the pubic symphysis, preventing delivery of the shoulder.
- This animation has pause and play buttons to allow for more interactivity during viewing.
-
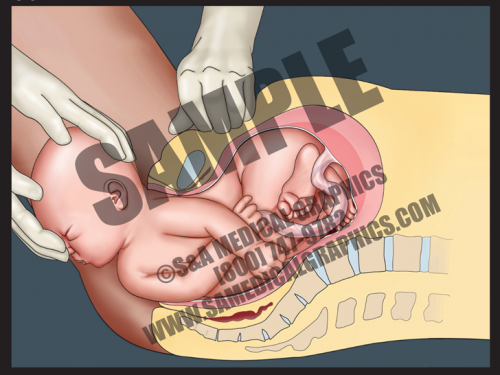
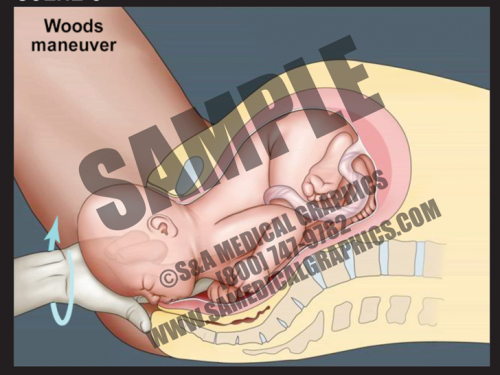
- This 2D dissolve animation shows how this maneuver can release shoulder dystocia impaction and allow for delivery of the fetal shoulder.
- Each animation has pause and play buttons to allow for more interactivity during viewing.
-
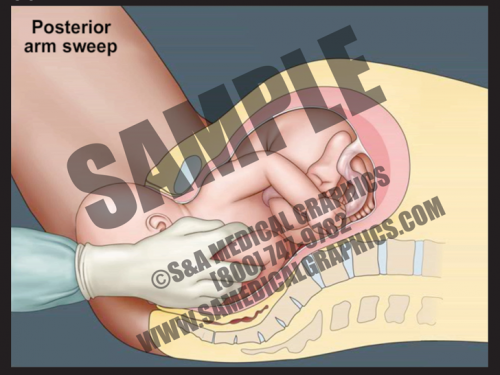
- This 2D dissolve animation shows how this maneuver can release shoulder dystocia impaction and allow for delivery of the fetal shoulder.
- Each animation has pause and play buttons to allow for more interactivity during viewing.
-
- This 2D dissolve animation shows how this maneuver can release shoulder dystocia impaction and allow for delivery of the fetal shoulder.
- Each animation has pause and play buttons to allow for more interactivity during viewing.
-
- This 2D dissolve animation shows how this maneuver can release shoulder dystocia impaction and allow for delivery of the fetal shoulder.
- Each animation has pause and play buttons to allow for more interactivity during viewing.
-
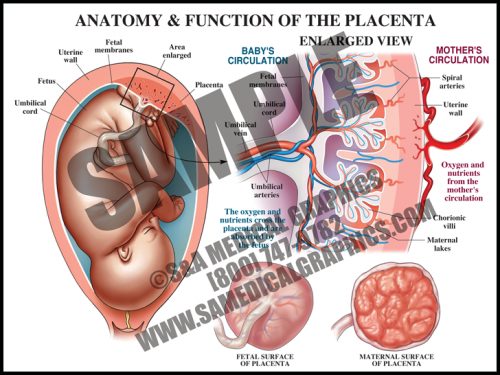
- The placental is a flattened, circular organ that develops in the uterus during pregnancy in order to support the fetus. The fetus is attached to the placenta via the umbilical cord.
- The placenta transfers oxygen and nutrients from the maternal blood to the fetal blood; it also transfers wastes products from the fetal blood to the maternal blood for removal.
- The umbilical cord is normally comprised of three blood vessels, two smaller umbilical arteries that carry deoxygenated blood from the fetus to the placenta, and a larger umbilical vein that supplies the fetus with oxygenated blood from the mother.
- The placenta is expelled from the uterus after the fetus is delivered. Placental pathology can reveal important information about intrauterine conditions and events, as well as shed light on the cause of adverse fetal outcome.
-
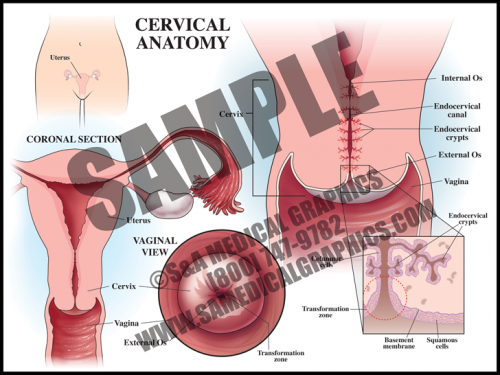
- The cervix is the circular muscle at the base of the uterus; it makes up the top of the vagina.
- The cervical canal passes through the cervix and allows blood from menstruation and a fetus to pass from the uterus into the vagina.
- During a pap smear, a screening test for cervical cancer, cells are scraped from the opening of the cervix and examined under a microscope for abnormality.
- The transformation zone is the area where the mucus secreting columnar cells of the endocervix meet the squamous cells of the ectocervix. Most squamous cell carcinomas and dysplasias are found here.
-
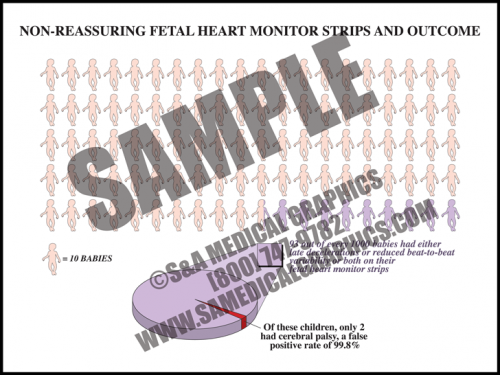
- One risk of fetal heart monitoring technology is false-positive results.
- In fact, “nonreassuring” FHM strips, or those which show either late decelerations, or reduced beat-to-beat variability, or both, have a greater than 99% false-positive rate in predicting cerebral palsy.
-
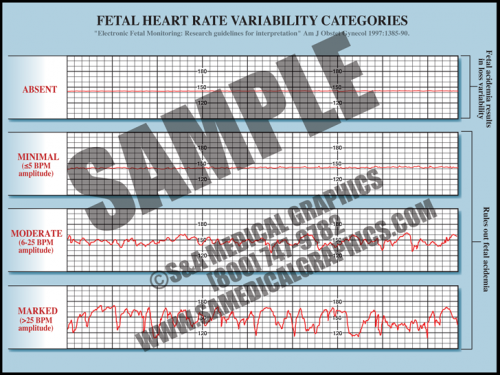
- Fetal heart rate is constantly varying from the baseline; this variability reflects a healthy fetal nervous system and cardiac responsiveness.
- These fluctuations are characterized as absent if there is no variation in the amplitude range, minimal if fluctuation is less than 5 bpm, moderate if fluctuation is 6 to 25 bpm, and marked if fluctuation is greater than 25 bpm.
- Absent variability indicates fetal academia but marked, moderate, and even minimal variation rules it out.
- Conditions like fetal hypoxia, congenital heart anomalies, and fetal tachycardia can cause a decrease in variability.
-
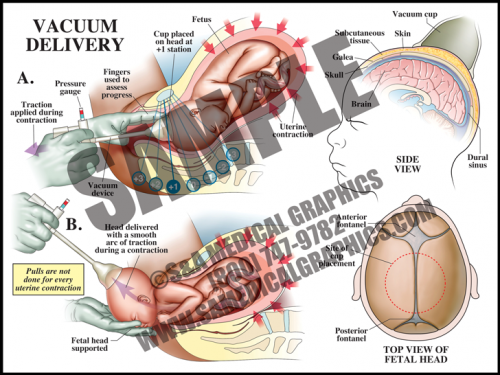
- Vacuum delivery may be performed in cases where there is a prolonged second stage of labor or suspicion of immediate or potential fetal compromise. This procedure assists delivery by helping to move the baby through the birth canal.
- The vacuum cap is a simple device that is placed on the vertex of the head with a small hand-held vacuum pump; some physicians leave the vacuum on between contractions and some release the vacuum. The caps are set to pop off if the vacuum pressure is too high.
- This procedure works with the uterine contractions, gently assisting and guiding the fetus out during contractions, and resting between them. It is not used between contractions.
-
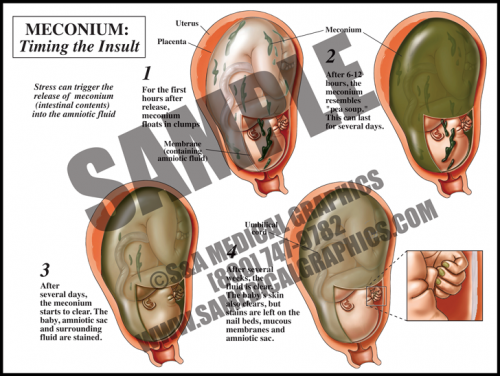
- Meconium is the dark, tarry contents of the fetal gastrointestinal tract. Meconium passage at labor and delivery is common and not a sign of fetal distress unless it is accompanied by other ominous signs.
- Meconium release into the amniotic fluid is however considered a sign of intrauterine fetal distress. This can be caused by placental insufficiency, maternal hypertension, and preeclampsia, among other things.
- When meconium is freshly released, it is clumpy and oats in the amniotic fluid. Within hours, it distributes particulate matter throughout the sac. Macrophages in the fetal skin, mucus membranes, and the amniotic sac phagocytize the particles, giving a green cast to the tissues.
- After several days, the fluid is greenish-brown but clear, and the fetus and membranes are stained. After several weeks, the fetal skin and fluid will clear, but the amniotic membranes, fetal mucus membranes, and nail beds remain stained.
-
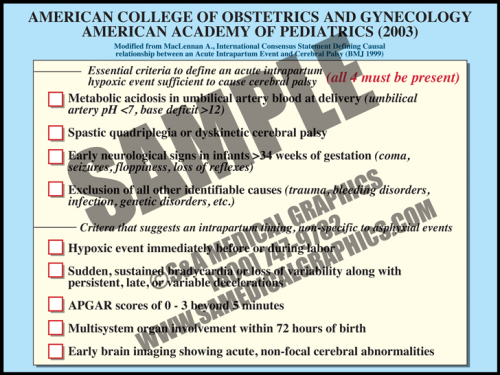
- In 2003, the American College of Obstetrics and Gynecology and the American Academy of Pediatrics recommended adoption of a definition of term intrapartum asphyxia developed by an international task force.
- The definition requires that all four parameters must be met in order to diagnose intrapartum asphyxiation in a term fetus. These include metabolic acidosis, diagnosis of specific types of cerebral palsy correlated with the types of asphyxia damage seen in term fetal brains, early seizures and other neurological signs, and exclusion of all other causes.
- There are other criteria that suggest an intrapartum timing of injury, nonspecific to asphyxia event. These include a hypoxic event immediately before or during birth, sudden, sustained bradycardia or loss of variability along with persistent, late, or variable decelerations, low APGAR scores (<3) beyond 5 minutes, multisystem organ involvement within 72 hours of birth, and early brain imaging showing acute, non-focal cerebral abnormalities.
-
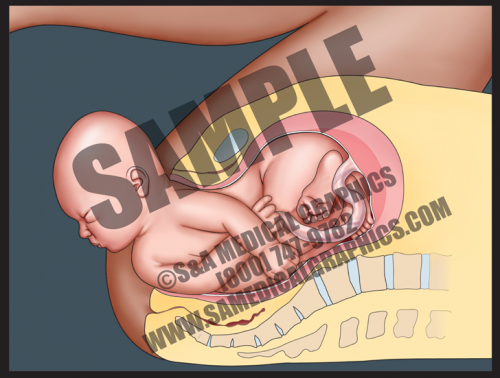
- In cases of shoulder dystocia, the upper fetal shoulder is impacted on the pubic symphysis, or more rarely, the lower shoulder becomes impacted on the sacral promontory or nonexible coccyx. In either case, this event prevents delivery of the baby. Shoulder dystocia can be a potentially catastrophic event since the fetal thorax is still within the pelvis and cannot properly expand for breathing.
- While the rate of shoulder dystocia is higher with gestational diabetic women and macrosomic fetuses (>4500 grams at birth), most cases of shoulder dystocia occur with average-sized fetuses.
- If a brachial plexus palsy (brachioplexopathy) occurs, it usually affects the portions of the brachial plexus that control the shoulder and elbow. Spontaneous recovery is the rule rather than the exception.
- Most fetuses are successfully delivered with a combination of McRoberts maneuver and suprapubic pressure.
-
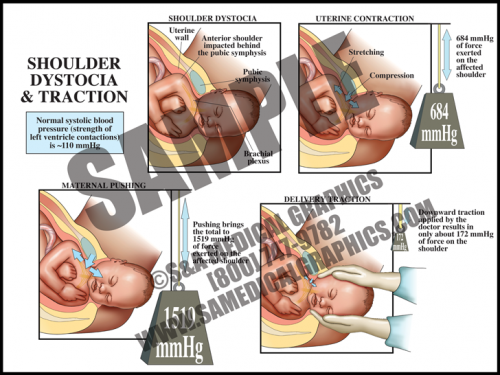
- The uterus itself generates tremendous pressure during contractions. If the average systolic blood pressure (pressure generated by the left ventricle during a contraction) is 120 mmHg, the uterus alone generates more than 5 times that amount. When the accessory muscles (the diaphragm and abdominal muscles) are used to push in conjunction with contractions, this pressure increases to more than 10 times that amount.
- The pull generated by a physician during downward traction for shoulder dystocia is slightly higher than the average systolic blood pressure and contributes only a very small amount to the total amount of generated pressures.
- Uterine and abdominal pressures are good evidence that if shoulder dystocia is the cause of brachial plexus palsy, it is most likely from the intrinsic pressures of the uterus and body wall, not the caregiver.
-
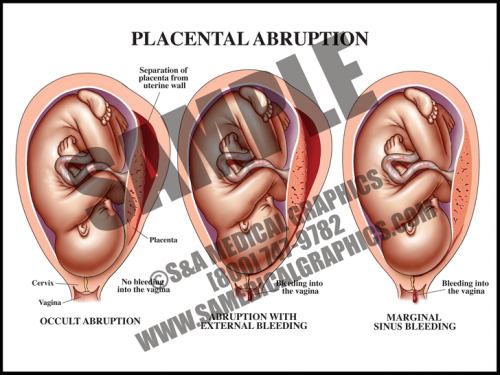
- Abruption occurs when the placenta separates from the uterine wall. Most of the time, this is accompanied by vaginal bleeding as the blood travels between the membranes and the uterus. Some- times, however, there is no bleeding because edges of the placenta remain sealed.
- Symptoms frequently include hypertonic uterus with severe abdominal pain and rapid contractions. If the abruption is large (more than about 50%), the fetus may not survive.
- The specific cause of placental abruption is often unknown, but risk factors include abdominal trauma and maternal factors like smoking, drinking, and diabetes, among others.
- Fetal distress occurs early in this condition in about half of all cases.
-
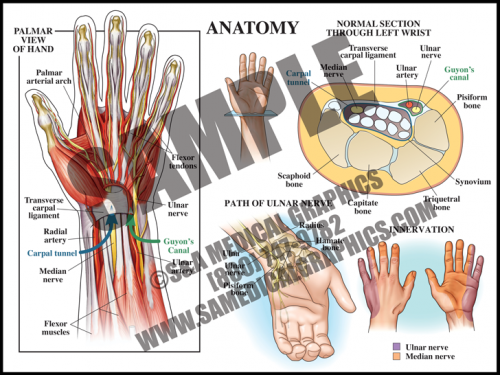
- The carpal tunnel is a passageway on the palmar side of the wrist that houses the median nerve and finger flexor tendons. Anteriorly, the carpal tunnel is bordered by the transverse carpal ligament, a heavy band of fibers that forms the fibrous sheath containing the carpal tunnel; posteriorly, the carpal tunnel is bordered by carpal bones.
- Guyon’s canal contains the ulnar nerve and artery; this anatomy does not pass through the tunnel, but lies superficial to it.
- Carpal tunnel syndrome occurs when the median nerve, which controls sensations to the palm side of the thumb, first, second, and half of the third finger, becomes compressed at the wrist, within the carpal tunnel. This results in pain, weakness, or numbness in the hand and wrist, radiating up to the arm.
-
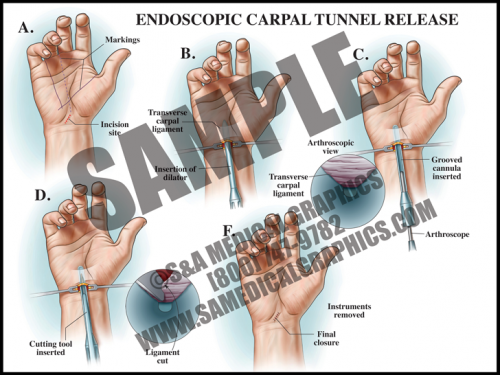
- If conservative treatment is not effective, surgical intervention may be chosen. Surgery can be done as an open procedure or endoscopically.
- In endoscopic surgery, a small incision is made in the wrist and a dilator tube is inserted. An arthroscope with a camera is inserted in order to view the anatomy, then a cutting tool is used to sever the transverse carpal ligament in order to reduce pressure on the median nerve.
- This type of surgery is less invasive and allows for faster recovery and less postoperative pain.
-
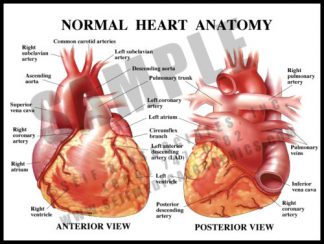
- Heart muscle is supplied by the coronary arteries, not by the blood flowing through the heart.
- The major coronary vessels are the right coronary artery (RCA) and left main coronary artery (LCA), both of which come directly off of the aorta via the coronary ostia.
- The LCA divides into the left anterior descending artery(LAD) and circumflex artery.
- The RCA has no major branches, and terminates as the posterior descending artery (PDA).
- There are may be variations in the anatomy.
-
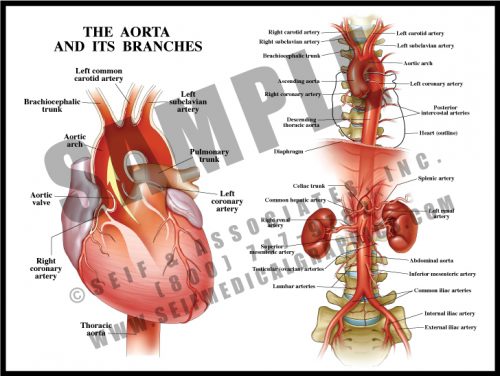
- The largest artery in the body, the aorta leaves the left ventricle and supplies all of the body’s tissues, including the heart itself, via its branches.
- The major parts are the arch (from the aortic valve to the left subclavian artery), descending thoracic aorta (from the left subclavian to the diaphragm) and abdominal aorta (from the diaphragm to the iliac bifurcation at about the level of the umbilicus).
- There are three major vessels leaving the arch and these supply the head, neck and arms; there are segmental vessels supplying the body wall throughout the length of the aorta. Major branches supply abdominal structures; the iliac arteries and their branches supply the pelvis and legs.
-
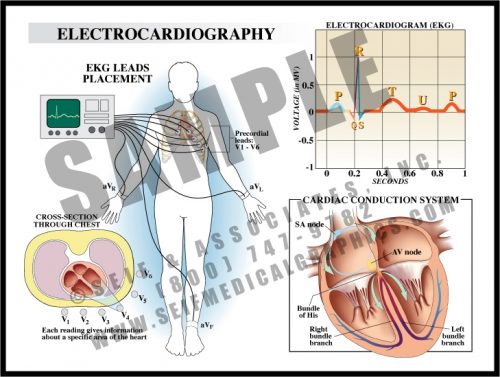
- A tracing is made from electrical impulses traveling through the heart, tracking the way the heart muscle reacts to the conduction system.
- An electrical impulse is initiated at the sinoatrial node, passes through specialized neuromuscular fibers lying beneath the inner lining of the heart until it reaches the atrioventricular node; from there, it travels through the Bundle of His, into the bundle branches and the Purkinje fibers, stimulating ventricular contraction.
- Changes in tracings are evaluated by comparing them to normal and/or baseline tracings; a physician can get information about areas of heart damage, both acute and chronic.
-
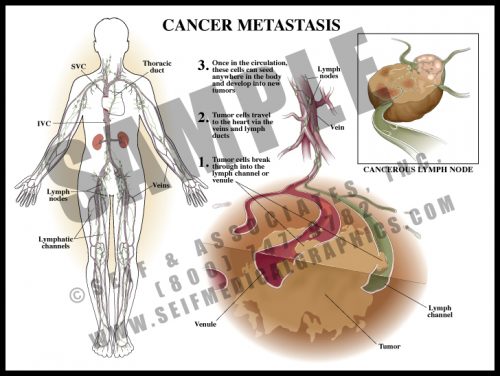
- Cancer tends to spread by two mechanisms: infiltration, in which the tumor pushes against and enters contiguous tissue; and metastasis, when cancer cells enter lymphatic channels and/or small blood vessels and eventually travel to distant locations and organs in the body.
- Certain tumors have a predilection for specific sites. Colon cancer frequently spreads to the liver, and breast cancer to the brain and spine.
- When there is lymphatic spread, the local and regional lymph nodes are the first line of defense; when the nodes fill up with dividing tumor cells, the cells then break free and travel toward the heart for distribution throughout the body.
-
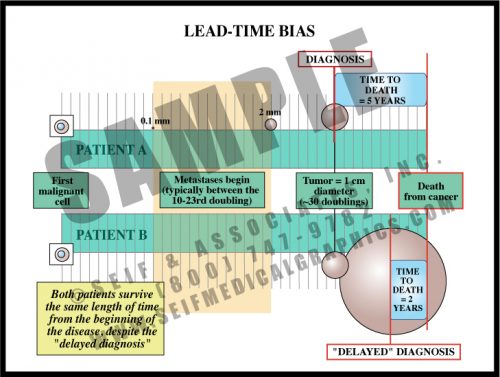
- A common assumption is that a cancer may not have been diagnosed early enough to make a difference, with the assumption being that early diagnosis is always better.
- In reality, cancers are present for very long periods of time before they are diagnosable, and many have metastasized prior to the period in which they can be detected.
- The life span of more than 60% of cancer patients is essentially predetermined by the characteristics of the cancer itself. While a patient diagnosed earlier may live “longer” than one diagnosed later, both patients actually survive about the same length of time from the first cancer cell.
-
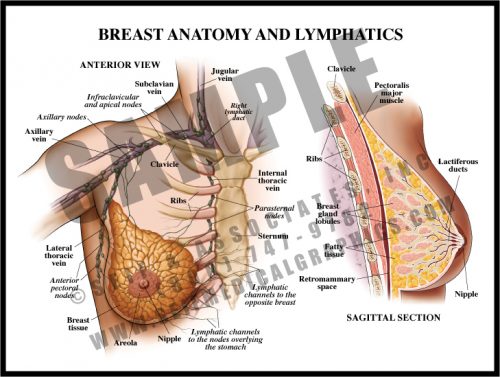
- The breast in a premenopausal woman is composed of glandular tissue, fat, connective tissue and ducts; the axillary tail of breast tissue is tucked upward in the axilla. The breast lies on the pectoralis muscles of the thorax.
- The breast is divided by irregular fibrous septa which prevent masses from migrating from one area of the breast to another; malignant tumors may eventually erode through these septa.
- Lymphatic channels travel throughout the breast, with all but the most medial portions draining to the axillary lymph nodes. The “sentinel” node—the first node to receive drainage from the breast—can be determined with testing and evaluated for metastatic spread.
- Post-menopausal women have little glandular tissue since most of it has been replaced by fat.
-
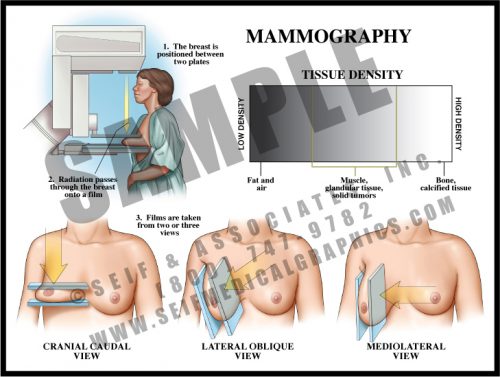
- Mammography is an imaging technique which allows visualization of breast tissue. Fat, glandular tissue and ductal tissue have characteristic densities and patterns.
- Solid tumors are generally easier to see in older patients with larger amounts of fat within the breasts, but can be difficult to see in patients with “dense” breasts (young women and women with fibrocystic breasts).
- Approximately 75% of breast cancers can be seen on mammography, with the patient’s breast characteristics being the largest determining factor.
-
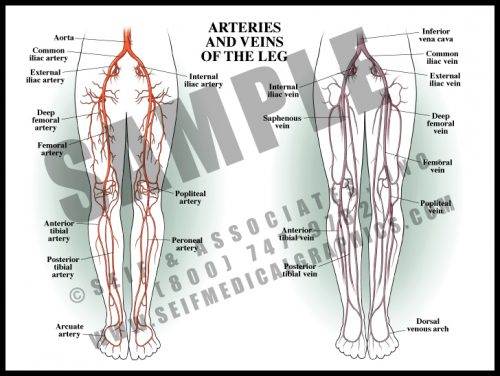
- Like in the arm, the deep, muscular arteries of the leg travel together, but the superficial veins are unpaired and variable in course.
- The legs receive blood from the terminal branches of the aorta, the iliac arteries. Branches supply the muscles of the thigh, and the name of the artery changes as it passes certain landmarks.
- The major vessels trifurcate behind the knee, dividing into the anterior and posterior tibial arteries and the peroneal artery, all of which travel toward the feet supplying the muscles and other tissues along the way.
- As in the arm, there are connective vascular arches in the foot supplying collateral circulation.
-
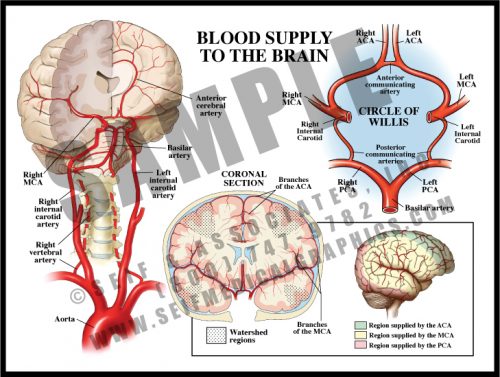
- The anterior 2/3 of the brain is supplied by branches of the internal carotid artery, whose terminal branches form the anterior and middle cerebral arteries.
- The vertebral arteries branch off the subclavian arteries and through small openings in the transverse processes of the cervical vertebrae. They merge to form the basilar artery supplying the cerebellum, brain stem, and the posterior cerebrum via the posterior cerebral arteries.
- The Circle of Willis has small connecting vessels between the three major cerebral vessels. Blood can change direction within the circle for collateral blood flow if needed. There can be significant variation in the form of the Circle of Willis from one individual to another.
- Tissues supplied by the tiny terminal branches of vessels are known as watershed regions and are vulnerable to damage during periods of low perfusion or oxygenation.
-
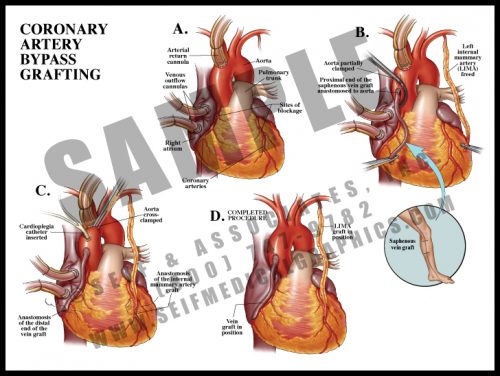
- When coronary arteries are significantly blocked (>70% stenosis), pain symptoms often occur with exercise in the form of stable angina, or at rest in the form of unstable angina.
- Bypass vessels are harvested as free grafts from the saphenous veins of the legs. These are anastomosed to the aorta and then to the coronary arteries, literally bypassing the blocked regions.
- The internal mammary arteries, which lie on either side of the sternum within the rib cage, can also be harvested and anastomosed directly to the coronary arteries. These grafts are less likely to stenose than are vein grafts.
- The procedure can be performed either on or off cardiopulmonary bypass.
-
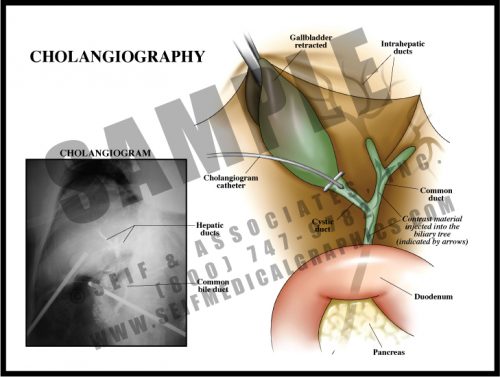
- Performed during surgery for gallbladder removal, this is an effective intraoperative radiographic test to look for either blockage or leakage in the biliary tree.
- This test may be performed prior to removing the gallbladder, or at any time a problem is suspected. A tiny catheter is threaded through a small incision in the cystic duct. Dye is injected into the biliary tract and x-rays are taken, allowing the surgeon to see which ducts are patent. Voids represent stones or tumors, and extravasation represents a leak in the system.
- While this test is very reliable in the case of a retained stone or suspected damage, the outcome in patients having routine intraoperative cholangiography without apparent complication is the same as those in whom the test was not performed.