This case involved a middle-aged male patient with bilateral inguinal hernias. The right side had both direct and indirect hernia, so the defendant repaired it with pre-cut mesh. The left side had smaller direct and indirect hernias, as well as an incarceration of a loop of the sigmoid. The defendant released the sigmoid colon and then used pre-cut mesh to repair this defect as well. Several weeks postoperatively, the patient began to complain of left groin burning and post-ejaculation testicular pain. His complaints varied over the next weeks, but then localized to pain in the right groin. The patient saw multiple doctors but his physical exams and multiple tests were essentially normal. His discomfort and minor urinary issues persisted and remained unrelieved by medications and trigger point injections.
About 15 months after the original surgery, the patient underwent a left inguinal hernia repair and division of the ilioinguinal nerve. During that procedure, adhesions were lysed and the ilioinguinal nerve was found to be adherent to the underside of the external oblique aponeurosis. The nerve was isolated and ligated proximally and distally to the entrapment. The hernia was repaired, the sigmoid was released, and the tissues were closed. The pathology was consistent with neuroma and the patient experienced relief of pain after the procedure for about 8 weeks.
The pain returned however and despite more trigger point injections and a number of visits to different physicians, he had no relief of pain or a diagnosis. He underwent mesh removal by another surgeon a year later, and shortly after he underwent a left orchiectomy. About three and a half years after the defendant’s original surgery, the patient underwent surgical removal of neuromas on the genitofemoral nerve, iliohypogastric nerve, and ilioinguinal nerve, embedding the proximal stumps in muscle.
The plaintiff alleged that the defendant improperly placed the mesh, resulting in damage to the splanchnic nerves on the vessels supplying the left testis. The defense contended that this patient was treated within the standard of care and that his postoperative problems were the result of nerve entrapment from adhesions.
The plaintiff alleged that the defendant improperly placed the mesh, resulting in damage to the splanchnic nerves on the vessels supplying the left testis.
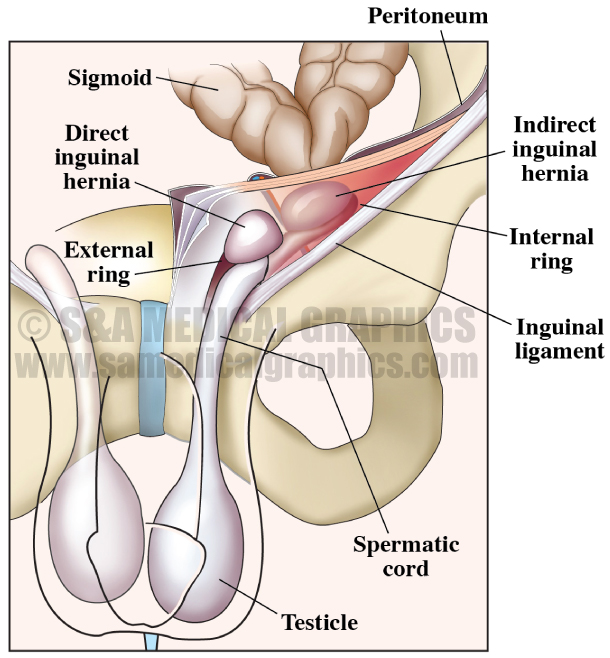
The first visual exhibit used in this case was designed to explain the anatomy of this patient’s hernia and to help the defendant explain to the jury what he encountered during surgery, how he repaired the hernia, and most importantly, how he placed the mesh.
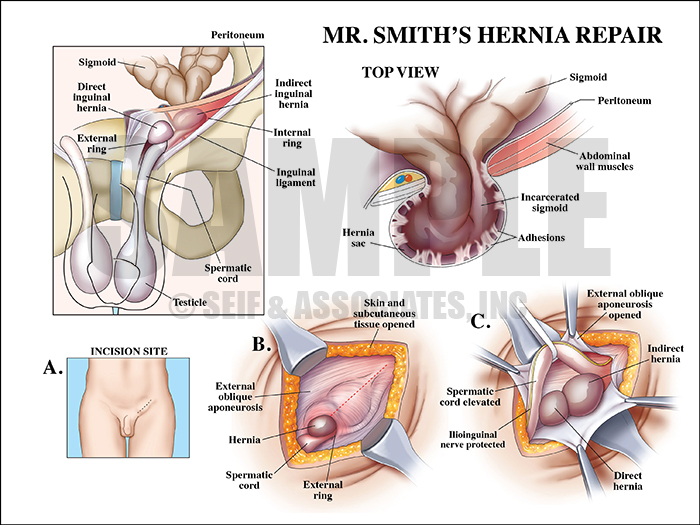
Exhibit 1 depicts the anatomy of the patient’s hernia during surgery.
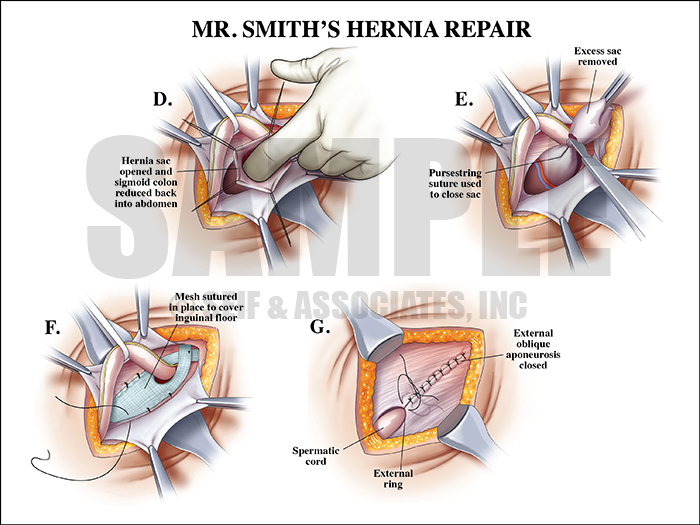
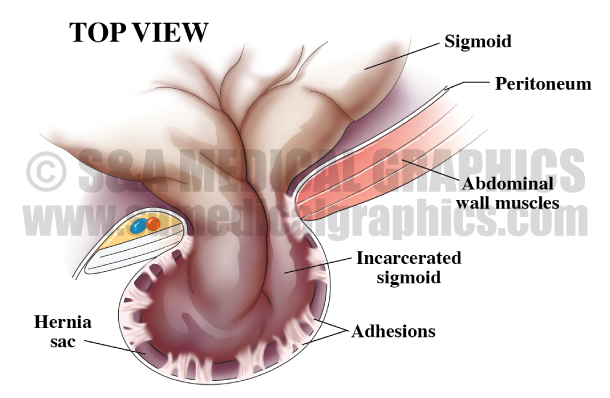
Exhibit 2 continues to depict the hernia repair surgery.
Once the jury could see that the procedure was performed within the standard of care, the next visual exhibit offered them an alternative explanation for the cause of this patient’s postoperative pain. The exhibit explains how adhesions form in the area after a surgical procedure, showing how they can encase and eventually distort and entrap the nerve, causing pain for the patient.
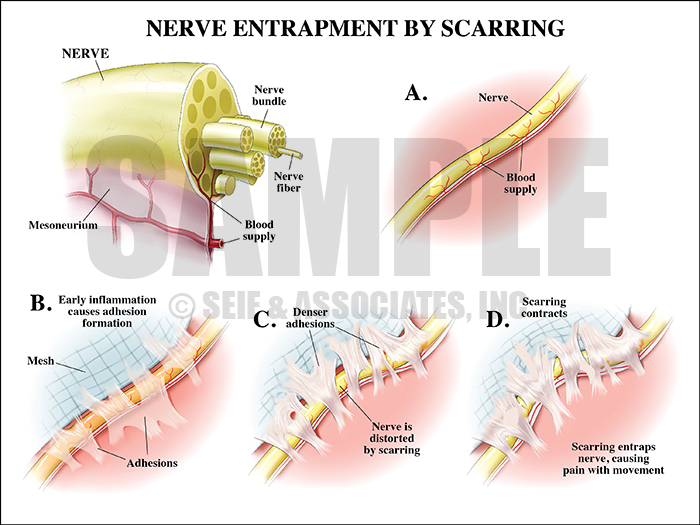
Exhibit 3 depicts how adhesions can encase and entrap nerves.
An overlay dropped down over this exhibit to further explain how adhesions can actually disrupt the blood supply of the nerve and result in the formation of a neuroma.
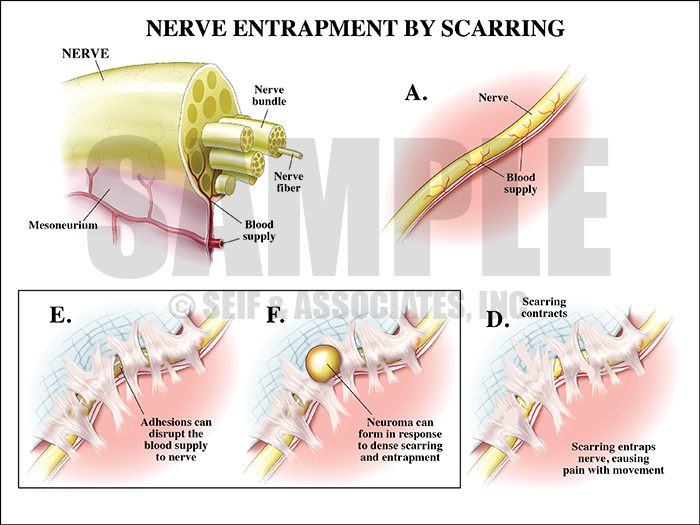
Overlay used during trial to explain how adhesions can cause a neuroma.
Overall the visual defense strategy in this case was to make sure that the jury understood that the defendant performed the patient’s surgery within the standard of care and there was no negligence. The visual exhibits then provided the jury an alternative cause and mechanism for this patient’s ongoing postoperative pain.
—Editorial contributed by Emily Ullo Steigler, MS, CMI
—Illustrations contributed by Robert Edwards, MS, CMI